

- Department of Neurosurgery, West Virginia University School of Medicine, Morgantown, West Virginia, USA
- Department of Radiology, West Virginia University School of Medicine, Morgantown, West Virginia, USA
Correspondence Address:
Sanjay Bhatia
Department of Neurosurgery, West Virginia University School of Medicine, Morgantown, West Virginia, USA
DOI:10.4103/sni.sni_351_16
Copyright: © 2017 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Roy S. Hwang, Ryan C. Turner, Walid Radwan, Rahul Singh, Brandon Lucke-Wold, Abdul Tarabishy, Sanjay Bhatia. Relationship of the sinus anatomy to surface landmarks is a function of the sinus size difference between the right and left side: Anatomical study based on CT angiography. 26-Apr-2017;8:58
How to cite this URL: Roy S. Hwang, Ryan C. Turner, Walid Radwan, Rahul Singh, Brandon Lucke-Wold, Abdul Tarabishy, Sanjay Bhatia. Relationship of the sinus anatomy to surface landmarks is a function of the sinus size difference between the right and left side: Anatomical study based on CT angiography. 26-Apr-2017;8:58. Available from: http://surgicalneurologyint.com/surgicalint-articles/relationship-of-the-sinus-anatomy-to-surface-landmarks-is-a-function-of-the-sinus-size-difference-between-the-right-and-left-side-anatomical-study-based-on-ct-angiography/
Date of Submission
23-Aug-2016
Date of Acceptance
07-Feb-2017
Date of Web Publication
26-Apr-2017
Abstract
Background:Several cadaveric studies demonstrate reliable localization of the transverse sinus and the transverse sigmoid junction (TSJ). These studies use the line drawn from the inion to the posterior root of the zygoma (IZ) and the asterion, respectively. We investigated how the size difference between the right and left transverse sinuses (TS) and sigmoid sinuses (SS) affected the accuracy of their respective superficial landmarks, particularly with regards to where this relationship may result in unsafe and/or complicated surgical access.
Methods:We utilized Vitrea software to render three-dimensional images based on computed tomographic angiography (CTA). We measured the relationship between the TS and SS to their respective superficial landmarks.
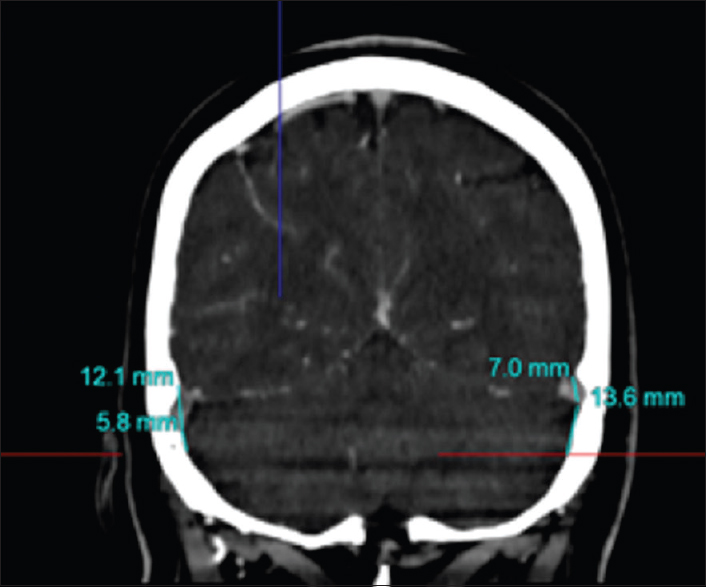
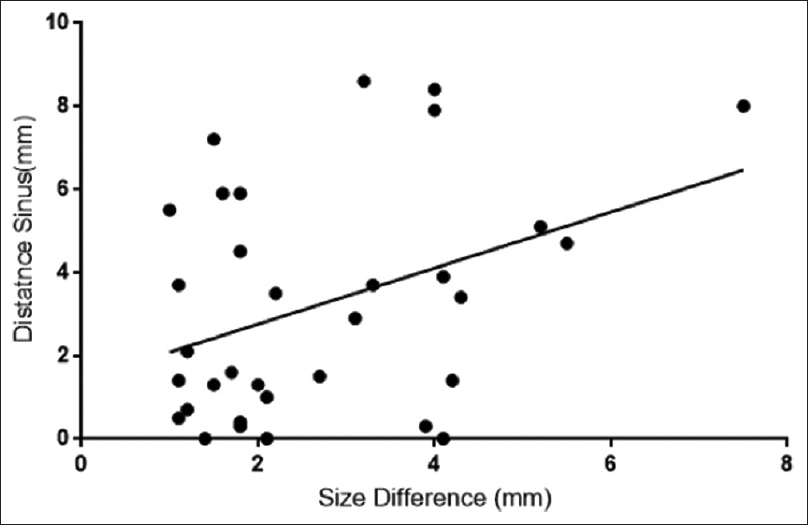
Results:We analyzed 50 patients in this study. The distal TS was found caudal to the inion-to-zygoma (IZ) line on average by 5.0 ± 4.3 mm on the right and 6.4 ± 9.3 mm on the left. The mid TS was found cranial on average 3.5 ± 5.7 mm on the right and 3.2 ± 6.0 mm cranial on the left to the superior nuchal line (SNL). The distance from the asterion to the SS was 11.5 ± 2.4 mm medial on the right and 12.1 ± 4.4 mm medial on the left. The average distance was greater on the left than the right when using the IZ landmark. This was directly proportional to the size difference of the sinuses (r2 = 0.15, P = 0.03).
Conclusions:Statistically significant differences between the right and left TS and SS were seen in terms of size. This appeared to correlate nicely to the differences observed between the locations of the TSs’ and their respective superficial landmarks.
Keywords: Computed tomography angiography, sinus location, surface anatomical landmarks, surgical planning
INTRODUCTION
The retrosigmoid craniotomy is the most common procedure used for the resection of cerebellopontine angle tumors (CPA).[
Each superficial landmark is associated with a specific section of the sinus anatomy. For example, the IZ line and the SNL approximates the TS, whereas the asterion approximates the TSJ. Studies disagree, however, on which landmarks are most important clinically.[
Our key objective was to measure the relationship between the known surface anatomical landmarks for the transverse sinus and transverse–sigmoid junction on both sides of the skull to determine the amount of variation between the right and left TS and their relationship to surface landmarks. We utilized volumetric 3D reconstruction of CT angiographic imaging to perform these analyses. The ultimate goal was to correlate and define the validity of CTA findings to known surface landmarks in order to guide: (1) Operative planning and (2) how to train neurosurgery residents in the importance of anatomical evaluation prior to entering the operative arena.
MATERIALS AND METHODS
We studied 50 consecutive patients who underwent CT angiographic imaging at our institution for various indications including transient ischemic attack, supratentorial intracranial hemorrhages, headaches, etc., Therefore, 100 anatomical sinuses were acquired for study (50 on the right-side and 50 on the left-side). Patients with posterior fossa lesions or a history of venous thrombosis were excluded from the study. Patients with imaging that was deemed inadequate for analysis were excluded from the study. General demographics such as age and sex were included for all studied patients.
Image acquisition
All images were obtained via multislice computed tomography (CT) angiography with iodine-based contrast, using an Aquilion CT scanner. Images were acquired under 1 mm thickness cuts. The CTA examinations in our institution were performed using an Aquilion ONE multidetector CT scanner (Toshiba Medical Systems, Japan), equipped with 320 × 0.5 mm detector rows covering 16 cubic cm of volume per rotation. The exam consists of a nonenhanced head CT (Kv 120, MA 240). The scan reformats in the standard three orthogonal planes followed by a CT angiogram with coverage from the skull base to the top of the head. This is done with an IV contrast range of 40 to 60 mL followed by a similar or smaller volume of saline chaser. The contrast is administered through an anticubital 18 to 20g IV at a rate of 4 to 5 mL/S. Images acquired from these acquisitions are automatically sent to PACS and to VITREA (Vitrea, Vital Images). The processed volumetric data is loaded directly into the VITREA system.
Study design and measurements
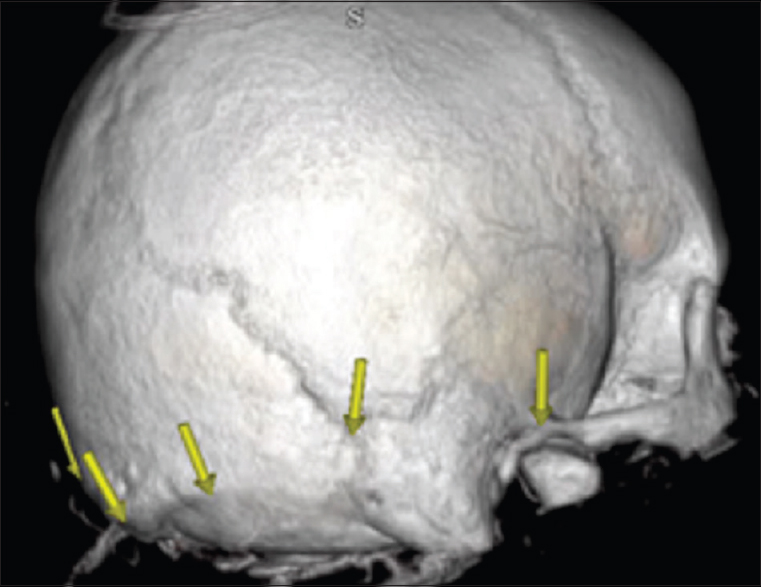
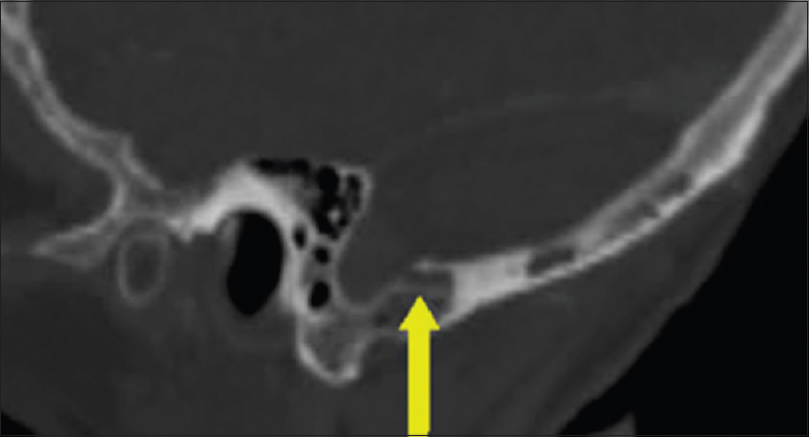
Two investigators performed VITREA 3D remodeling of the images and performed measurements based on the 3D volumetric model and multiplanar reconstructions. The plane of the inion to the posterior root of the zygoma (IZ) as well as the superior nucal line (SNL) were localized and identified. The asterion was identified as the junction between the lambdoid, occipitomastoid, and parietomastoid sutures. The SNL was identified as the superior bony protuberance in direct continuity with the inion [
Statistical analysis
All measurements were studied using statistical software GraphPad Prism 7.0 with a P value less than 0.05 indicating statistical significance. Student's t-test was used to compare the means, and Chi-square analysis was utilized for proportional analyses. A linear regression analysis was used to compare the relationship between the differences in size of the left and right sinuses and its relative distance to the overlying superficial landmark.
RESULTS
Of the 50 patients and 100 half skulls analyzed, the average size of the TS and SS was greater on the right (9.2 vs 8.4 mm) than the left (11.2 vs 10.4 mm). This was statistically significant (P-value = 0.04, 0.03, respectively). The plane defined by the IZ line was on average 5.0 mm caudal on the right and 6.4 mm caudal on the left to the lower border of the distal TS just before the TSJ at the location of the asterion for both the right and left sides. The SNL was on average cranial to the lower border of the mid TS on the right and left sides. The sigmoid sinus was lateral to the asterion about 11.2 mm right and 12.1 mm on the left [

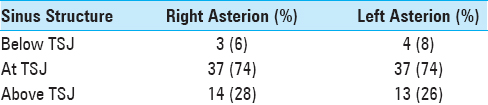
Interestingly, the TSJ was below the asterion in 14 patients on the right (28%) and 13 patients on the left (26%). No statistical significance was observed between the right and left sides [

The average distance from the superficial landmarks was greater on the left than the right when using the inion to the zygoma landmark and greater on the right when using the SNL as a landmark. This appeared to be a function of the size of the sinuses. On regression analyses, a relationship between the size of the sinus and its proximity to the superficial landmarks was found. This was statistically significant, although with a modest correlation coefficient (r2 = 0.15, P = 0.03) [
DISCUSSION
There have been several studies performed utilizing cadavers to localize the sinus anatomy focusing on a single side of the skull during a lateral suboccipital craniotomy.[
Several other studies have shown close approximation of CT and MR imaging to what is seen intraoperatively on a single side of the skull.[
Our main objective for this study was to delineate the difference between the left and right TS position and size as they correlate with bony landmarks. This is an important consideration for neurosurgeons and adds value especially when planning the surgical approach. We found that the right and left TS were invariably different in size and the right TS was more often larger than the left TS. We found a modest but statistically significant correlation between the size difference and the distance to the superficial landmark. As has been delineated in prior studies, no single landmark was completely accurate. The mid and proximal TS were closest to the SNL and its lower margin was often found below it. The SNL did not correspond to the IZ line, and the IZ line was always found below the SNL. Therefore, the TS roughly courses between the SNL and the IZ line as it moves distally from the proximal/mid TS segment to the distal TS. The lower edge of the TS is roughly 5 mm above IZ line at the level of the asterion, and none of the measured sinuses were found to be more than 5 mm below the IZ line just before the asterion. The TSJ is approximated at the asterion in roughly 74% of the patients in our study, and the SS courses inferiorly approximately 1 cm lateral to the asterion. It is important for neurosurgical residents to carefully consider these anatomical correlations and know how they differ between the left and right side as outlined in the following paragraph.
If one is operating on the right side, the sinus tends to be larger, and therefore, the landmark is either more cranial to the SNL or less caudal to the IZ line during bone removal [
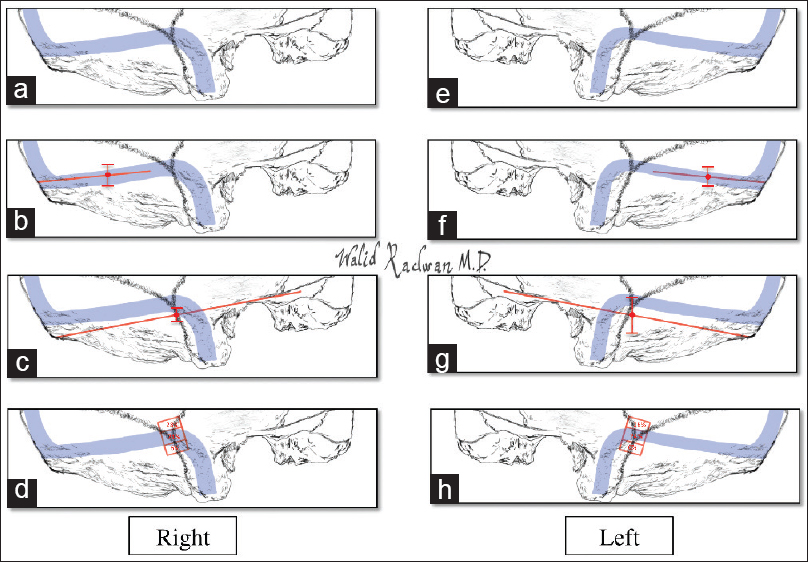
Figure 5
Artist illustration of predicted course of TS and TSJ right and left Both right (a) and left (e) TS and TSJ drawn to scale. Average location of TS in reference to the superior nuchal line with range shown on right (b) and left (f). Average location of TS in reference to the IZ line with range shown on right (c) and left (g). Average location of TSJ in reference to the asterion with range shown on right (d) and left (h). The most common predicted course of the TS was closely related to the SNL at the TS proximal and mid segment. The distal TS prior to the TSJ was most likely found above the IZ line before the asterion. The asterion localized the TSJ approximately 80% of the time. The sigmoid sinus was roughly 1 cm distal to the caudal line drawn below the asterion
A limitation of this study is the potential for measurement error given the restriction of measurements within a single plane. In comparison, in a dry or fixed cadaver skull measurements can be made in multiple planes simultaneously, as one takes a ruler that can encircle the skull in three dimensions. The key benefit of this work, however, is that we expanded upon the initial work of Sheng et al. by examining the differences between the TSs’ on the right and left independently. This is important because it directs the neurosurgeon to a safe placement of the burr hole depending on the side of the skull being operated on. We strongly advocate for further studies to use imaging processing software in studying surgical anatomy. This will not only aid in greater appreciation of anatomical differences but also provide a powerful tool for operative planning.
CONCLUSION
In conclusion, we describe a method that enables us to measure the anatomical relationship between superficial landmarks and their associated underlying vascular structures (sinuses) via volumetric 3D rendering of CT angiographic imaging. This method is proven to have good correlation to prior anatomical studies.[
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Avci E, Kocaogullar Y, Fossett D, Caputy A. Lateral posterior fossa venous sinus relationships to surface landmarks. Surg Neurol. 2003. 59: 392-7
2. Bozbuga M, Boran BO, Sahinoglu K. Surface anatomy of the posterolateral cranium regarding the localization of the initial burr-hole for a retrosigmoid approach. Neurosurg Rev. 2006. 29: 61-3
3. da Silva EB, Leal AG, Milano JB, da Silva LF, Clemente RS, Ramina R. Image-guided surgical planning using anatomical landmarks in the retrosigmoid approach. Acta Neurochir. 2010. 152: 905-10
4. Day JD, Kellogg JX, Tschabitscher M, Fukushima T. Surface and superficial surgical anatomy of the posterolateral cranial base: Significance for surgical planning and approach. Neurosurgery. 1996. 38: 1079-83
5. Day JD, Tschabitscher M. Anatomic position of the asterion. Neurosurgery. 1998. 42: 198-9
6. Gharabaghi A, Rosahl SK, Feigl GC, Samii A, Liebig T, Heckl S. Surgical planning for retrosigmoid craniotomies improved by 3D computed tomography venography. Eur J Surg Oncol. 2008. 34: 227-31
7. Han H, Yao Z, Wang H, Deng X, Yu Fong AH, Zhang M. Dural entrance of the bridging vein into the transverse sinus provides a reliable measure for preoperative planning: An anatomic comparison between cadavers and neuroimages. Neurosurgery. 2008. 62: ONS289-95
8. Kivelev J, Kivisaari R, Niemela M, Hernesniemi J. Muscle Insertion Line as a Simple Landmark To Identify the Transverse Sinus When Neuronavigation Is Unavailable. World Neurosurg. 2016. 94: 394-7
9. Raso JL, Gusmao SN. A new landmark for finding the sigmoid sinus in suboccipital craniotomies. Neurosurgery. 2011. 68: 1-6
10. Ribas GC, Rhoton AL, Cruz OR, Peace D. Suboccipital burr holes and craniectomies. Neurosurg Focus. 2005. 19: E1-
11. Samii M, Matthies C. Management of 1000 vestibular schwannomas (acoustic neuromas): The facial nerve--preservation and restitution of function. Neurosurgery. 1997. 40: 684-94
12. Sheng B, Lv F, Xiao Z, Ouyang Y, Lv F, Deng J. Anatomical relationship between cranial surface landmarks and venous sinus in posterior cranial fossa using CT angiography. Surg Radiol Anat. 2012. 34: 701-8
13. Tubbs RS, Loukas M, Shoja MM, Bellew MP, Cohen-Gadol AA. Surface landmarks for the junction between the transverse and sigmoid sinuses: Application of the “strategic” burr hole for suboccipital craniotomy. Neurosurgery. 2009. 65: S37-41
14. Tubbs RS, Salter G, Oakes WJ. Superficial surgical landmarks for the transverse sinus and torcular herophili. J Neurosurg. 2000. 93: 279-81
15. Ucerler H, Govsa F. Asterion as a surgical landmark for lateral cranial base approaches. J Craniomaxillofac Surg. 2006. 34: 415-20

