

- Department of Neurosurgery, Takeda General Hospital, Fushimiku, Kyoto, Japan.
Correspondence Address:
Masahiro Kawanishi
Department of Neurosurgery, Takeda General Hospital, Fushimiku, Kyoto, Japan.
DOI:10.25259/SNI_688_2020
Copyright: © 2020 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Masahiro Kawanishi1, Yutaka Ito1, Hidekazu Tanaka1, Kunio Yokoyama1, Makoto Yamada1, Akira Sugie1. Resolution of retro-odontoid cyst in a patient with atlanto-occipital assimilation after occipitocervical fixation. 28-Jan-2021;12:34
How to cite this URL: Masahiro Kawanishi1, Yutaka Ito1, Hidekazu Tanaka1, Kunio Yokoyama1, Makoto Yamada1, Akira Sugie1. Resolution of retro-odontoid cyst in a patient with atlanto-occipital assimilation after occipitocervical fixation. 28-Jan-2021;12:34. Available from: https://surgicalneurologyint.com/surgicalint-articles/10549/
Date of Submission
01-Oct-2020
Date of Acceptance
14-Oct-2020
Date of Web Publication
28-Jan-2021
Abstract
Background: Fusion of the atlas with the lower part of the occiput is clinically known as atlanto-occipital assimilation (AOA) or atlas occipitalization. This can be either partial or complete depending on the extent of fusion. AOA is one of the most common congenital anomalies of the craniovertebral junction and is usually asymptomatic.
Case Description: An 80-year-old female presented with a retro-odontoid cyst in conjunction with AOA. Following posterior occipitocervical fixation without resection of the cyst, the patient improved, and the postoperative MR documented cyst resolution.
Conclusion: Patients with AOA and a retro-odontoid cyst may be successfully managed with occipitocervical fixation without resection of the cyst. However, we would recommend preoperative computed tomography angiography to document whether the vertebral artery follows an anomalous course to avoid an intraoperative neurovascular injury.
Keywords: Assimilation, Occipitocervical fusion, Retroodotoid pseudo tumor
INTRODUCTION
Atlas occipitalization or atlanto-occipital assimilation (AOA) is one of the most common osseous congenital anomalies of the craniovertebral junction.[
Here, we described a case in which AOA associated with a retro-odontoid cyst was successfully fused, resulting in spontaneous regression of the cyst.
CASE REPORT
An 80-year-old female was admitted with progressive gait disturbance, and weakness of the upper extremities of 6 months’ duration. She demonstrated a useless right hand, a spastic quadriparesis, and diffuse hyperreflexia, accompanied by bilateral Babinski signs.
The dynamic X-rays showed AOA without atlantoaxial instability, while the sagittal MR demonstrated a retroodontoid cystic mass compressing the spinal cord [
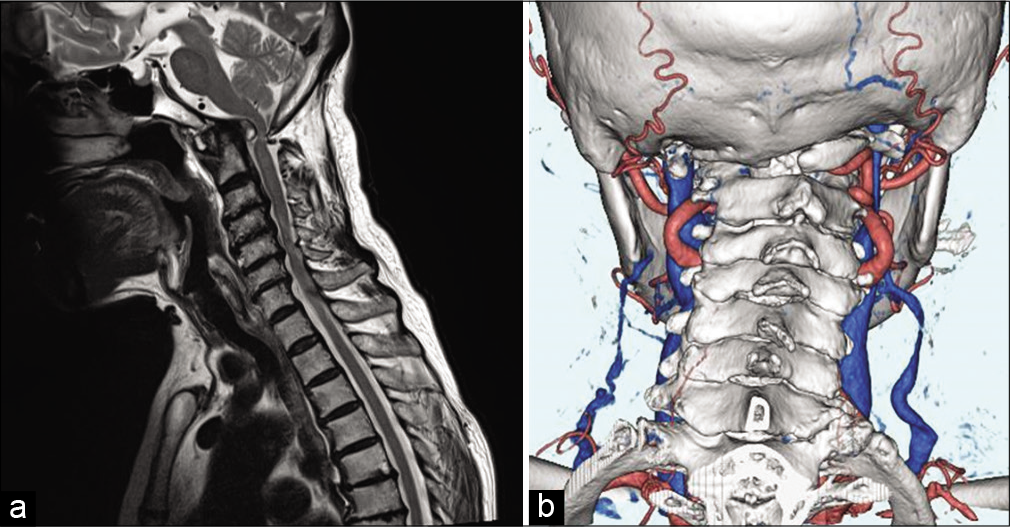
Figure 1:
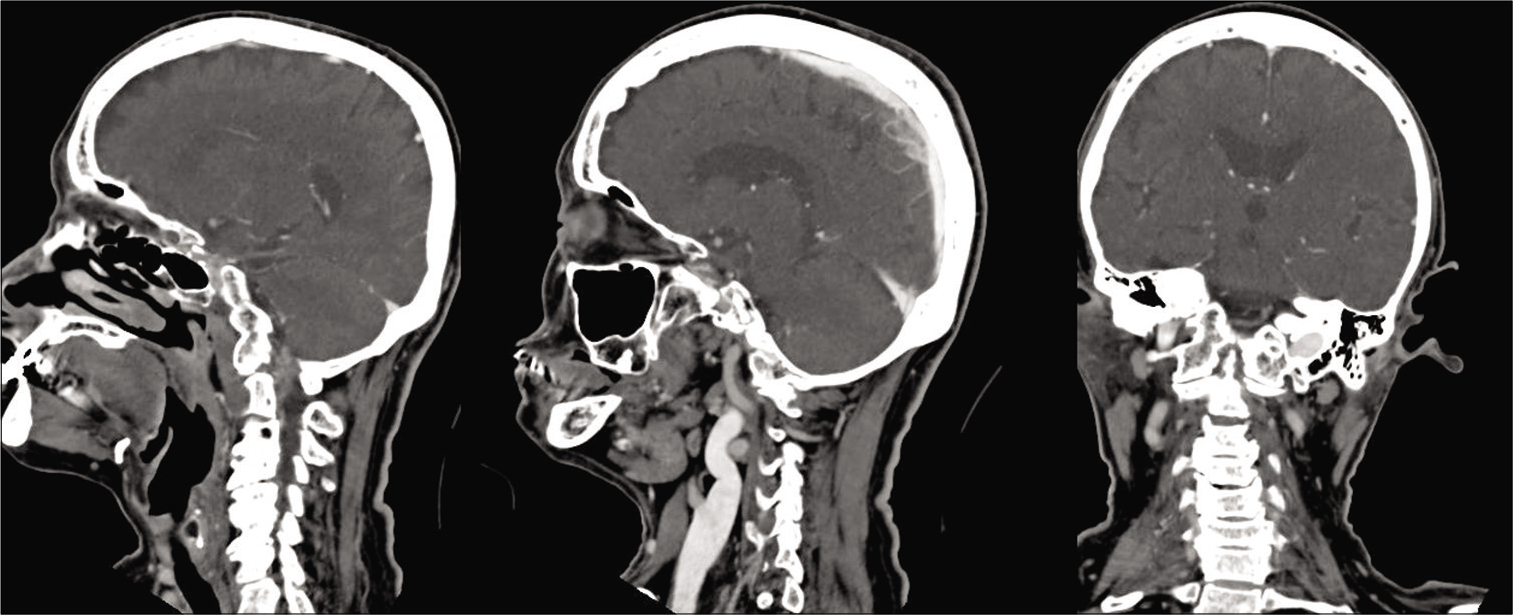
(a) Sagittal T2-WI revealed retro-odontoid cystic mass compressing the spinal cor. (b) Posterior view of three-dimensional computed tomography clearly demonstrates an assimilation with agenesis of the left VA and right VA entering the spinal canal below the occipitalized C1 posterior arch [Figures 1b and 2].
Operation
An occiput–C2 fusion was performed. Screws were secured to the occipital bone while C2 pedicle screws were applied; fixation then consisted of connection of the two with bilateral rods; and the fusion construct then included placement of structural iliac bone grafts affixed with smaller screws [
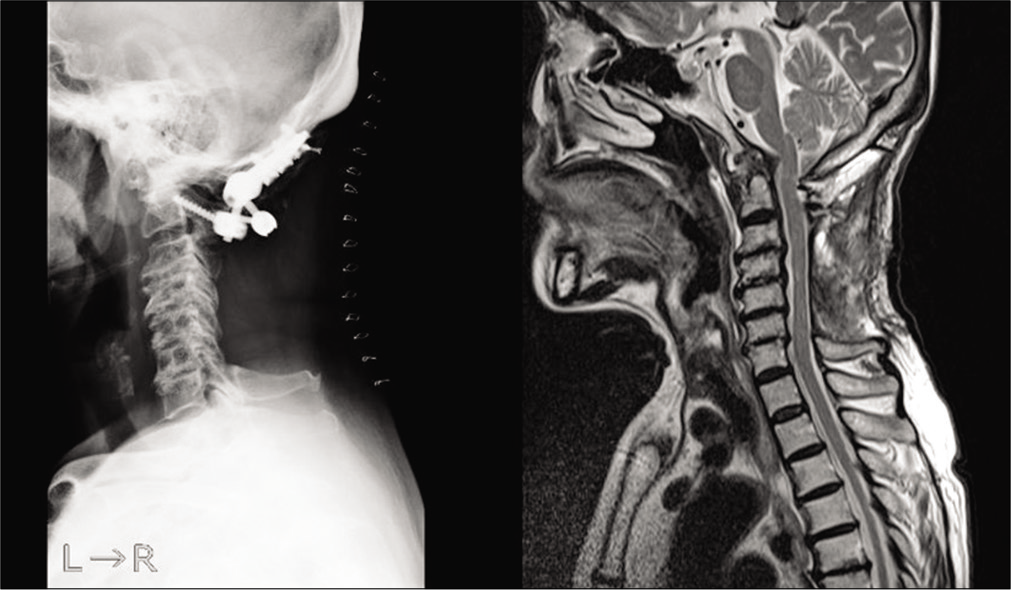
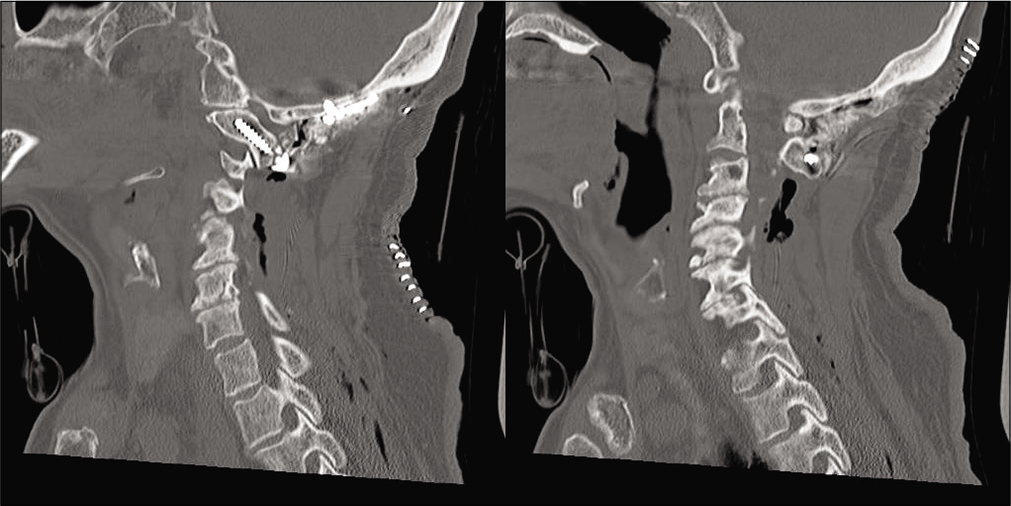
Postoperative course
Within 3 postoperative months, she regained normal strength, and the follow-up MR revealed moderate regression of the retroodontoid cystic mass [
DISCUSSION
Congenital assimilation of the atlas (AOA) is caused by the failure of segmentation between the last occipital, and first cervical sclerotome during the early fetal development.[
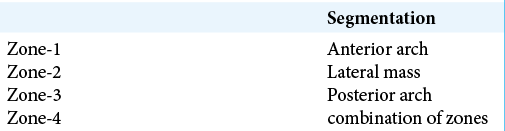
Table 1:
Failure segmentation parts (Gholve et al.).[
Symptomatic versus asymptomatic AOA
AOA is often asymptomatic, except where occipitalization results in fixation of both atlanto-occipital joints that bear more than 50% of the flexion/ extension motion.[
Association with anomalous VA
Patients with AOA may demonstrate an abnormal course of the VA involving its third segment. Our patient had such an anomaly of the right VA. Wang et al. reported four distinct types of VA anomalies associated with occipitalization of the atlas [
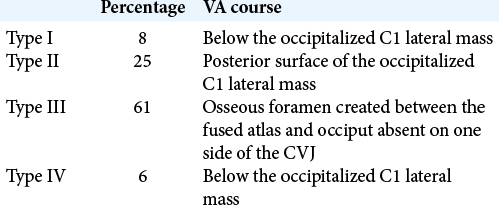
Table 2:
Four types of VA at craniovertebral junction (Wang et al.).[
CONCLUSION
Patients with AOA and a retro-odontoid cyst may be successfully managed with occipitocervical fixation without resection of the cyst. However, we would recommend preoperative computed tomography angiography to document whether the vertebral artery follows an anomalous course to avoid an intraoperative neurovascular injury.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Burke SM, Huhta TA, Mackel CE, Riesenburger RI. Occipital condyle fracture in a patient with occipitalisation of the atlas. BML Case Rep. 2015. 2015: bcr2015209623
2. Gholve PA, Hosalkar HS, Ricchetti ET, Pollock AN, Dormans JP, Drummond DS. Occipitalization of the atlas in children, Morphologic classification, associations, and clinical relevance. J Bone Joint Surg Am. 2007. 89: 571-8
3. Khamanarong K, Woraputtaporn W, Ratanasuwan S, Namking M, Chaijaroonkhanarak W, Sae-Jung S. Occipitalization of the atlas: Its incidence and clinical implications. Acta Med Acad. 2013. 42: 41-5
4. Lang J.editors. Skull Base and Related Structures: Atlas of Clinical Anatomy. New York, Stuttgart: Schattauer; 1995. p. 54
5. Lu K, Lee TC. Spontaneous regression of periodontoid pannus mass in psoriatic atlantoaxial subluxation. Case report. Spine (Phila Pa 1976). 1999. 24: 578-81
6. Macalister A. Notes on the development and variations of the Atlas. J Anat Physiol. 1893. 27: 519-42
7. Mudaliar RP, Shetty S, Nanjundaiah K, Kumar JP, Kc J. An osteological study of occipitocervical synostosis: Its embryological and clinical significance. J Clin Diagn Res. 2013. 7: 1835-7
8. Offiah CE, Day E. The craniocervical junction: Embryology, anatomy, biomechanics and imaging in blunt trauma. Insights Imaging. 2017. 8: 29-47
9. Sharma DK, Sharma D, Sharma V. Atlantooccipital fusion: Prevalence and its developmental and clinical correlation. J Clin Diagn Res. 2017. 11: AC01-3
10. Soni P, Sharma V, Sengupta J. Cervical vertebrae anomalies-incidental findings on lateral cephalograms. Angle Orthod. 2008. 78: 176-80
11. Wang S, Wang C, Liu Y, Yan M, Zhou H. Anomalous vertebral artery in craniovertebral junction with occipitalization of the atlas. Spine (Phila Pa 1976). 2009. 34: 2838-42
12. Yamaguchi I, Shibuya S, Arima N, Oka S, Kanda Y, Yamamoto T. Remarkable reduction or disappearance of retroodontoid pseudotumors after occipitocervical fusion, Report of three cases. J Neurosurg Spine. 2006. 5: 156-60

