

- Department of Vascular Neurosurgery, Instituto Nacional de Neurología y Neurocirugía “Manuel Velasco Suárez,” Ciudad de México, Mexico.
Correspondence Address:
Edgar Nathal, Department of Vascular Neurosurgery, Instituto Nacional de Neurología y Neurocirugía “Manuel Velasco Suárez,” Ciudad de México, Mexico.
DOI:10.25259/SNI_678_2022
Copyright: © 2022 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Alejandro Serrano-Rubio, Bill Roy Ferrufino-Mejia, Juan C. Balcázar-Padrón, Héctor A. Rodríguez-Rubio, Edgar Nathal. Ruptured aneurysm associated with a twig-like middle cerebral artery: An illustrative case report. 07-Oct-2022;13:456
How to cite this URL: Alejandro Serrano-Rubio, Bill Roy Ferrufino-Mejia, Juan C. Balcázar-Padrón, Héctor A. Rodríguez-Rubio, Edgar Nathal. Ruptured aneurysm associated with a twig-like middle cerebral artery: An illustrative case report. 07-Oct-2022;13:456. Available from: https://surgicalneurologyint.com/?post_type=surgicalint_articles&p=11922
Date of Submission
28-Jul-2022
Date of Acceptance
01-Sep-2022
Date of Web Publication
07-Oct-2022
Abstract
Background: Anomalies of the middle cerebral artery (MCA) are rare; among the different types of anomalies, the aplastic or twig-like (Ap/T) MCA is extremely rare and has been reported under various names, including aplastic, unfused, or rete type anomaly. The occurrence of a brain aneurysm associated with this anatomic variant is an even rare event, and probably their development and rupture are related to hemodynamic stress of the tinny wall of vessels forming the network.
Case Description: We present a 43-year-old male patient with an explosive and persistent right orbitofrontal headache. A computed tomography showed a right frontobasal hematoma with intraventricular disruption. Magnetic resonance angiography showed a right MCA aneurysm and what seems to be a MCA trunk stenosis. Cerebral digital subtraction angiography demonstrated a plexiform arterial network and one aneurysm arising from the network. The patient was successfully treated by surgical clipping to evacuate the hematoma and to prevent further intracranial hemorrhages.
Conclusion: The Ap/T-MCA may be associated with hemodynamic stress with a significant effect through the tinny wall of the vessels causing hemorrhage or leading to the formation and rupture of cerebral aneurysms. Based on a correct diagnosis of the anomaly, treatment can be completed successfully through different standard methods.
Keywords: Aneurysm, Clipping surgery, MCA anomaly, Middle cerebral artery, Twiglike MCA
INTRODUCTION
Aplastic or twig-like middle cerebral artery (Ap/T-MCA), also called “unfused MCA,” “rete MCA” or “anomalous collateral artery,” is a rare anatomic anomaly with a very low prevalence among population (0.11–0.88%),[
CASE DESCRIPTION
This 43-year-old male with a history of systemic arterial hypertension was admitted to the hospital because a sudden onset of severe headache of 7 days evolution accompanied by nausea, vomiting, and a right-side hemiparesis.
Computed tomography (CT) revealed a frontobasal hematoma with ventricular disruption [
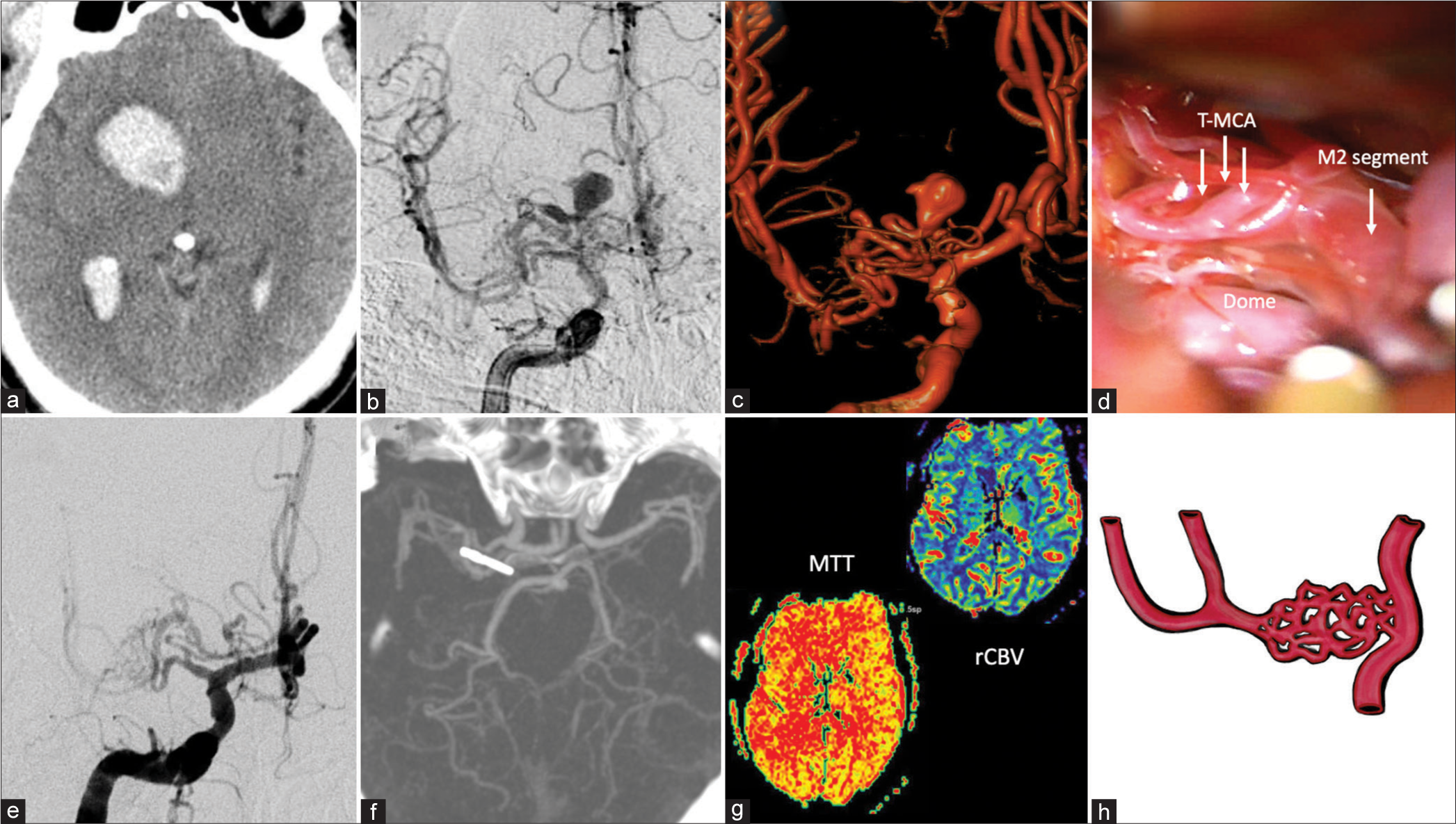
Figure 1:
Illustrative case (a) A right frontobasal hematoma with ventricular extension is seen on noncontrast Computed tomography (CT) scan. (b and c) Cerebral DSA with rotational 3-D show the presence of a saccular aneurysm in the middle of the vascular network. (d) Intraoperative view. After evacuating the hematoma, the vascular network is exposed (T-MCA). Under the superficial vessels of the anomaly, the dome of the aneurysm is just visible. Distal M2 segment seems normal. (e) Postoperative DSA. The aneurysm is not visible. (f) CT-angio displays the clip position and the complete exclusion of the aneurysm. (g) Perfusion MRI showing the mean transit time (MTT) and regional cerebral blood volume (rCBV) images without ischemic areas (h) Illustration of the Ap/T MCA anomaly depicting the plexiform arterial network replacing the proximal M1 segment.
The patient was operated on 3 weeks after ictus, through a right side pterional approach. After opening the Sylvian fissure, the vessels network was visualized, formed by numerous tinny and fragile vessels, with the aneurysm located in the middle of this network with old clots and hemosiderin surrounding the lesion [
A straight 7 mm Yasargil type clip was used for neck clipping. We verified total occlusion using intraoperative fluorescein videoangiography and intraoperative Doppler. The postoperative course was uneventful and the patient showed a total recovery of the initial preoperative neurologic deficit in the next days. Postoperative cerebral DSA and CT- angio showed the disappearance of the aneurysm without associated low-density areas [
Video 1
DISCUSSION
Ap/T-MCA is a rare vascular anomaly. It has been considered that embryological interruption of the MCA trunk genesis is the cause, being replaced by the formation of a plexiform arterial anomaly [
Due to the difficulty of diagnosing this anomaly on noninvasive imaging modalities such as CT and MR angiography, it is often misdiagnosed as arteriovenous malformation or pseudo-occlusion of the MCA. In patients that underwent a DSA, the Ap/T-MCA was present 0.11% and 1.17% of them.[
Akkan et al. described three types of “Ap/T-MCA” presentations, where the entire MCA is composed of a vascular network; in another presentation, the vascular network terminates at the bifurcation. In the last case, the vascular plexiform network ends before the beginning of the bifurcation.[
The twig-like appearance of the vessels may be confused with the MMD; however, there is no evidence of a progressive internal carotid artery occlusion leading to the formation of the Moyamoya vessels, as occurs in MMD.[
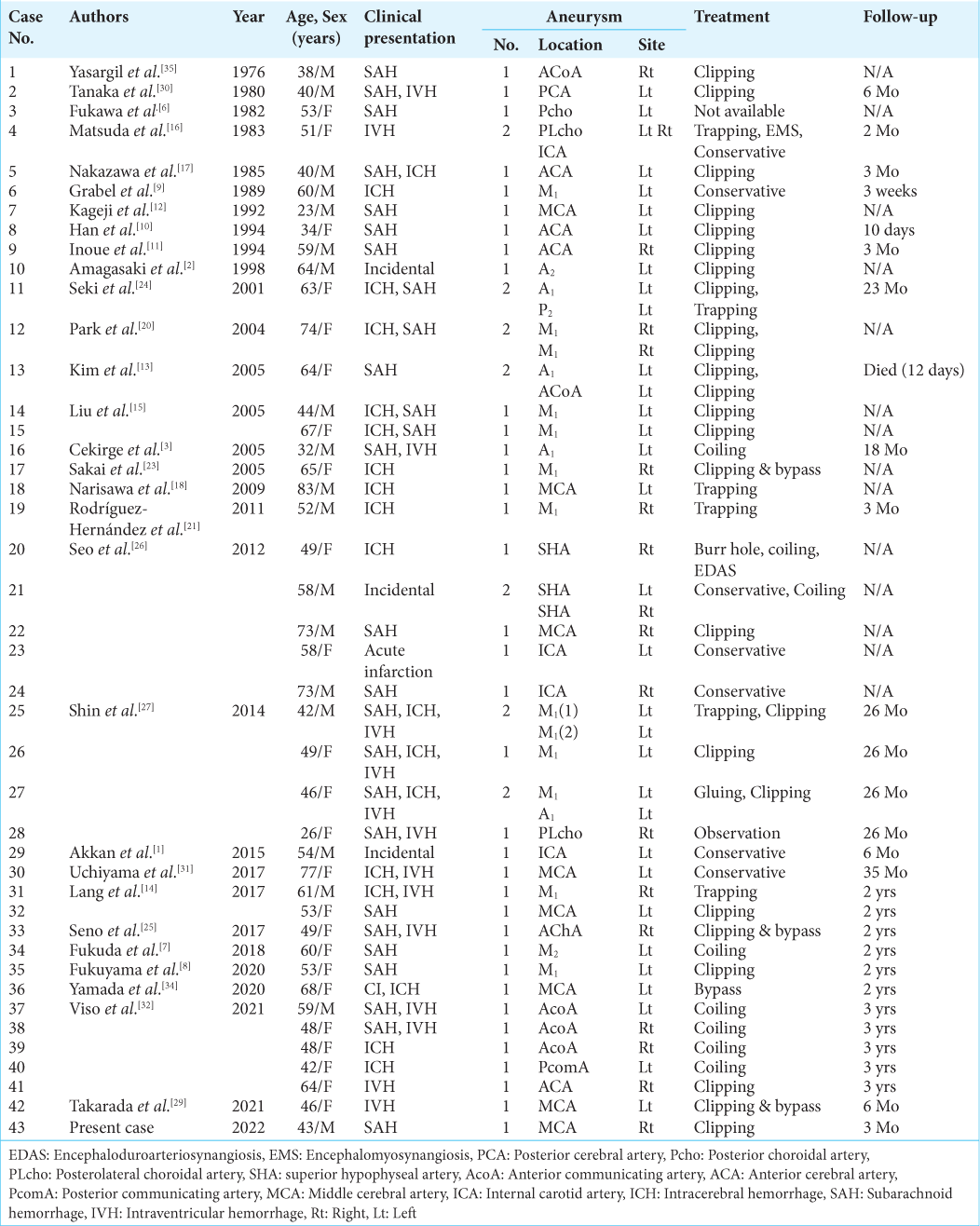
At present, there are 42 cases in the international literature of aneurysms associated with the Ap/T-MCA anomaly, of which 26 presented as SAH,[
In this case, our patient had a Fisher Grade IV subarachnoid hemorrhage. During surgery, after evacuating the surrounding hematoma, we found many fragile vessels of the network around the aneurysm that bleed easily. Compression of the bleeding points with surgical patties quickly stopped the hemorrhage without the need of cauterization with the bipolar forceps, assuming the thrombotic mechanism of the vessel.
Ap/T-MCA can present with hemorrhagic stroke in 27–40% of the cases, of which up to 26.6–46% were associated with aneurysm rupture. On the other hand, ischemic stroke can be present in 33–46% of cases.[
Endovascular coil embolization and surgical clipping are procedures that have been associated with success in managing ruptured aneurysms. However, in the presence of a hematoma causing a mass effect, as occurred in this case, the surgical approach is mandatory. Endovascular coiling has been used mainly in aneurysms located lateral to the twig-like anomaly. In cases associated with ischemic events, cerebral revascularization surgery may be used whenever a perfusion study was done showing hypoperfusion in the MCA territory of the Ap/T-MCA. In our case, this procedure was unnecessary since there were not ischemic events or neurological deficits.[
CONCLUSION
The Ap/T-MCA is a rare anomaly. There is a lack of knowledge and information about it due to the scarcity of reports in the literature. However, when present, it should be diagnosed correctly to avoid unnecessary therapeutic considerations in patients with acute symptomatology. DSA remains as the gold standard for diagnoses. The occurrence of cerebral aneurysms associated with this anomaly requires additional considerations. In case of unruptured aneurysms, an endovascular or surgical procedure has been reported as effective methods, but in ruptured cases associated with brain hematomas, surgical treatment is mandatory. This case gives rise to a complete opening in both diagnosis and treatment of aneurysms in variants of the MCA as the twig-like type. More detailed clinical studies with a large population are required to determine the optimal treatment of Ap/T-MCA associated with aneurysms or ischemic events.
Videos available on:
Declaration of patient consent
Patient’s consent not required as patient’s identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Akkan K, Ucar M, Kilic K, Celtikci E, Ilgit E, Onal B. Unfused or twig-like middle cerebral artery. Eur J Radiol. 2015. 84: 2013-8
2. Amagasaki K, Yagishita T, Kawataki T, Kase M, Nukui H. Middle cerebral artery aplasia associated with an aneurysm of the proximal anterior cerebral artery. Acta Neurochir (Wien). 1998. 140: 1313-4
3. Cekirge HS, Peynircioglu B, Saatci I. Endovascular treatment of an “anterior cerebral artery” aneurysm in a patient with “embryonic unfused middle cerebral artery” anomaly: A case report. Neuroradiology. 2005. 47: 690-4
4. Cho KC, Kim JJ, Jang CK, Hong CK, Joo JY, Kim YB. Rete middle cerebral artery anomalies: A unifying name, case series, and literature review. J Neurosurg. 2018. 131: 453-61
5. Cho WS, Kim JE, Kim CH, Ban SP, Kang HS, Son YJ. Long-term outcomes after combined revascularization surgery in adult moyamoya disease. Stroke. 2014. 45: 3025-31
6. Fukawa O, Aihara H, Wakasa H. Middle cerebral artery occlusion with moyamoya phenomenon--2nd report: Report of an autopsy case. No Shinkei Geka. 1982. 10: 1303-10
7. Fukuda Y, Matsunaga Y, Hirayama K, Yoshimura S, Somagawa C, Satoh K. A case of aplastic or twig-like middle cerebral artery associated with a ruptured A1 aneurysm at the origin of the anomalous collateral artery. Jpn J Stroke. 2018. 40: 75-80
8. Fukuyama R, Yamamura K, Murata H, Miyatake S, Matsumoto N, Abe H. Ruptured aneurysm of an aplastic or twig-like middle cerebral artery with ring finger protein 213 mutation: A case report. No Shinkei Geka. 2020. 48: 533-40
9. Grabel JC, Levine M, Hollis P, Ragland R. Moyamoya-like disease associated with a lenticulostriate region aneurysm. Case report. J Neurosurg. 1989. 70: 802-3
10. Han DH, Gwak HS, Chung CK. Aneurysm at the origin of accessory middle cerebral artery associated with middle cerebral artery aplasia: Case report. Surg Neurol. 1994. 42: 388-91
11. Inoue A, Kohno K, Fukumoto S, Ichikawa H, Onoue S, Miyazaki H. A case of ECA-MCA double anastomoses for hemorrhagic type of Twig-Like MCA. No Shinkei Geka. 2016. 44: 463-71
12. Kageji T, Murayama Y, Matsumoto K. Spontaneous middle cerebral artery occlusion with moyamoya-like vessels associated with contralateral middle cerebral artery aneurysm; A case report. No Shinkei Geka. 1992. 20: 177-81
13. Kim MS, Oh CW, Hur JW, Lee JW, Lee HK. Aneurysms located at the proximal anterior cerebral artery and anterior communicating artery associated with middle cerebral artery aplasia: Case report. Surg Neurol. 2005. 64: 534-7
14. Lang M, Moore NZ, Witek AM, Kshettry VR, Bain MD. Microsurgical repair of ruptured aneurysms associated with moyamoya-pattern collateral vessels of the middle cerebral artery: A report of two cases. World Neurosurg. 2017. 105: 1042.e5-10
15. Liu HM, Lai DM, Tu YK, Wang YH. Aneurysms in twig-like middle cerebral artery. Cerebrovasc Dis. 2005. 20: 1-5
16. Matsuda M, Handa J, Saito A, Matsuda I, Kamijyo Y. Ruptured cerebral aneurysms associated with arterial occlusion. Surg Neurol. 1983. 20: 4-12
17. Nakazawa T, Suzuki F, Miyamoto Y, Matsuda M. Aplasia of the proximal middle cerebral artery associated with an aneurysm of the proximal anterior cerebral artery. Case report. Nihon Geka Hokan. 1985. 54: 521-5
18. Narisawa A, Takahashi T, Saito R, Sato K, Endo H, Noshita N. A case of repeated intracerebral hemorrhage due to a ruptured aneurysm of collateral circulation from the posterior cerebral artery to the middle cerebral artery. No Shinkei Geka. 2009. 37: 787-92
19. Pagiola I, Abaurre L, Pianca P, Pimentel D, Barbosa L. Twig-like middle cerebral artery: A rare condition not to be confused with Moyamoya disease. Arq Neuropsiquiatr. 2021. 79: 1043-6
20. Park J, Hwang JH, Hamm IS. Aneurysm rupture at an anomalous collateral artery that extended from the proximal A2 segment to the middle of the M1 segment, bypassing atresia of the internal carotid artery bifurcation. Case report. J Neurosurg. 2004. 100: 332-4
21. Rodríguez-Hernández A, Lu DC, Miric S, Lawton MT. Aneurysms associated with non-moyamoya collateral arterial networks: Report of three cases and review of literature. Neurosurg Rev. 2011. 34: 517-22
22. Sahu CD, Bhargava N, Sahana D, Kumar S. Rete middle cerebral artery anomaly presenting with a large intracerebral hemorrhage: A case report. J Clin Interv Radiol. 2021. 6: 147-9
23. Sakai K, Hiu T, Fukuda Y, Ozono K, Honda K, Kawahara I. A rare case of a ruptured de novo aneurysm arising from the twig-like networks of an anomalous collateral artery associated with hypoplasia of the M1 segment of the middle cerebral artery 4 years after the rupture of an A1 aneurysm at the origin of the collateral artery. No Shinkei Geka. 2018. 46: 713-22
24. Seki Y, Fujita M, Mizutani N, Kimura M, Suzuki Y. Spontaneous middle cerebral artery occlusion leading to moyamoya phenomenon and aneurysm formation on collateral arteries. Surg Neurol. 2001. 55: 58-62 discussion 62
25. Seno T, Kohno K, Tanaka H, Iwata S, Fukumoto S, Ichikawa H. A case of ruptured distal anterior choroidal artery aneurysm associated with a twig-like middle cerebral artery, treated with single-stage aneurysm clipping and STA-MCA double anastomoses in the acute phase. No Shinkei Geka. 2017. 45: 691-7
26. Seo BS, Lee YS, Lee HG, Lee JH, Ryu KY, Kang DG. Clinical and radiological features of patients with aplastic or twiglike middle cerebral arteries. Neurosurgery. 2012. 70: 1472-80 discussion 1480
27. Shin HS, Lee SH, Ryu CW, Koh JS. Flow-related intracranial aneurysms associated with unfused arterial twigs relevant to different vascular anomalies: Embryologic and hemodynamic considerations. Acta Neurochir (Wien). 2014. 156: 1637-46
28. Shirokane K, Tamaki T, Kim K, Morita A. Subarachnoid hemorrhage attributable to bilateral aplastic or twiglike middle cerebral artery. World Neurosurg. 2020. 134: 560-3
29. Takarada A, Yanaka K, Onuma K, Nakamura K, Takahashi N, Ishikawa E. Aplastic or twig-like middle cerebral artery harboring unruptured cerebral aneurysms treated by clipping and bypass surgery: Illustrative case. J Neurosurg Case Lessons. 2021. 2: CASE21360
30. Tanaka Y, Takeuchi K, Akai K. Intracranial ruptured aneurysm accompanying moyamoya phenomenon. Acta Neurochir (Wien). 1980. 52: 35-43
31. Uchiyama T, Okamoto H, Koguchi M, Tajima Y, Suzuyama K. A case of aplastic or twig-like middle cerebral artery presenting with an intracranial hemorrhage two years after a transient ischemic attack. No Shinkei Geka. 2016. 44: 143-8
32. Viso R, Lylyk I, Albiña P, Lundquist J, Scrivano E, Lylyk P. Hemorrhagic events associated with unfused or twig-like configuration of the middle cerebral artery: A rare vascular anomaly with clinical relevance. Interv Neuroradiol. 2021. 27: 285-90
33. Watanabe N, Marushima A, Hino T, Minamimoto S, Sato M, Ito Y. A ruptured aneurysm in aplastic or twig-like middle cerebral artery: A case report with histological investigation. NMC Case Rep J. 2022. 9: 7-12
34. Yamada D, Ishibashi R, Kinosada M. Aplastic or twig-like middle cerebral artery with short-term ischemia and bleeding. Jpn J Stroke. 2020. 42: 190-5
35. Yaşargil MG, Smith RD. Association of middle cerebral artery anomalies with saccular aneurysms and moyamoya disease. Surg Neurol. 1976. 6: 39-43

