

- Department of Neurosurgery, Kouzenkai Yagi Neurosurgical Hospital, Osaka, Japan
- Department of Neuro-Intervention, Osaka City General Hospital, Osaka, Japan
- Department of Neurosurgery, Osaka Medical and Pharmaceutical University Hospital, Takatsuki, Japan.
Correspondence Address:
Seigo Kimura, Department of Neurosurgery, Kouzenkai Yagi Neurosurgical Hospital, Osaka, Japan.
DOI:10.25259/SNI_507_2023
Copyright: © 2023 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Seigo Kimura1, Masaki Komiyama2, Hirokatsu Taniguchi1, Masahiko Wanibuchi3. Ruptured small cerebral aneurysm occurring at the fenestration of the A1 portion of the anterior cerebral artery, combined with accessory middle cerebral artery branching from the crus: A case report. 01-Sep-2023;14:311
How to cite this URL: Seigo Kimura1, Masaki Komiyama2, Hirokatsu Taniguchi1, Masahiko Wanibuchi3. Ruptured small cerebral aneurysm occurring at the fenestration of the A1 portion of the anterior cerebral artery, combined with accessory middle cerebral artery branching from the crus: A case report. 01-Sep-2023;14:311. Available from: https://surgicalneurologyint.com/surgicalint-articles/12520/
Date of Submission
15-Jun-2023
Date of Acceptance
18-Aug-2023
Date of Web Publication
01-Sep-2023
Abstract
Background: Cerebral aneurysms arising from fenestration of the A1 portion of the anterior cerebral artery (ACA) (A1 fenestration) with the accessory middle cerebral artery (MCA) is rare. Herein, we report a ruptured cerebral aneurysm arising from A1 fenestration combined with the accessory MCA that was successfully treated with coil embolization.
Case Description: A 51-year-old woman suddenly experienced a severe occipital headache and was admitted to our hospital. Detailed examination revealed subarachnoid hemorrhage due to a cerebral aneurysm arising from A1 fenestration combined with the accessory MCA. Hence, coil embolization was performed, and a favorable outcome was obtained.
Conclusion: Coil embolization of the cerebral aneurysm arising from the A1 fenestration of the ACA combined with the accessory MCA is considered to be useful.
Keywords: Accessory middle cerebral artery, Anterior cerebral artery, Coil embolization, Fenestration, Subarachnoid hemorrhage
INTRODUCTION
Fenestration of the A1 portion (A1 fenestration) of the anterior cerebral artery (ACA) is a variation that forms in the embryonic period,[
CASE REPORT
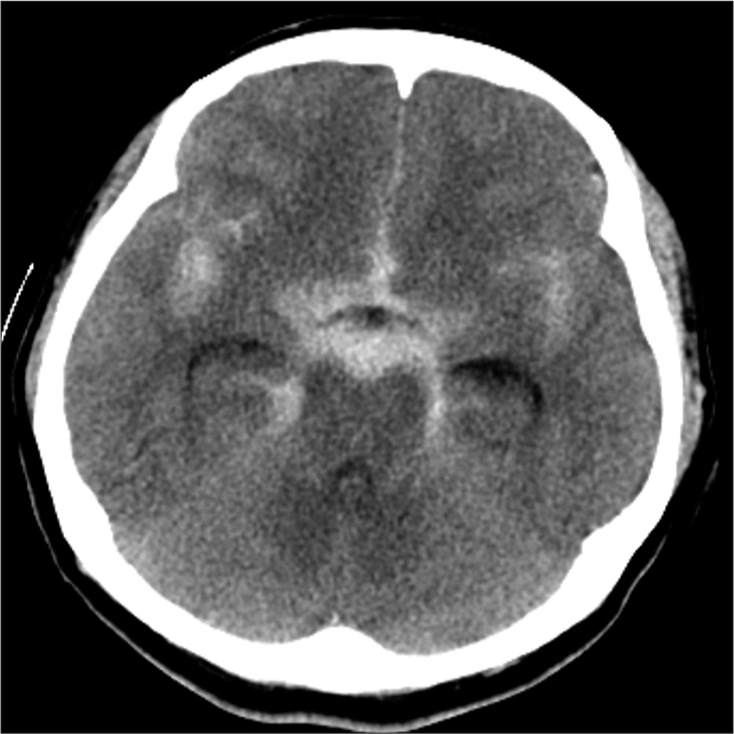
A 51-year-old woman suddenly experienced an occipital headache and collapsed at home. Her family contacted emergency medical assistance, and she was admitted to our hospital. She had a history of hypertension, but her family history was insignificant. On arrival at our hospital, her Glasgow Coma Scale score was 15 (E4, V5, and M6) with no apparent paresis. However, she had a severe occipital headache. Her blood pressure level and pulse rate were 192/99 mmHg and 95/min, respectively. Head computed tomography (CT) revealed a subarachnoid hemorrhage (Fisher group 3) [
DISCUSSION
In 1905, Fawcett and Blachford reported an A1 fenestration incidence of 0.14%.[
Surgical treatment for cerebral aneurysms associated with A1 fenestration includes clipping and coil embolization. For cerebral aneurysms associated with A1 fenestration, 25 cases of clipping and ten cases of coil embolization have been reported in previous studies; furthermore, reports of coil embolization are increasing.[
A1 fenestration tends to cause tunica media defects at the proximal end. Therefore, it has been reported that the majority of cerebral aneurysms that occur in the A1 fenestration occur at the proximal end of the fenestration due to hemodynamic stress.[
In the present case, the vascular structure around the cerebral aneurysm was complex, and clipping was thought to be difficult. In addition, the diameter of the cerebral aneurysm was small and the risk of hemorrhagic complications from coil embolization was high.[
CONCLUSION
Herein, we report a ruptured cerebral aneurysm arising from the A1 fenestration combined with the accessory MCA that was successfully treated with coil embolization. Hemodynamic stress toward ACA and accessory MCA may have added to the tunica media defect of the proximal end of the A1 fenestration, which may have influenced the occurrence of a cerebral aneurysm. Although the vascular structure was complex and the cerebral aneurysm was small, detailed imaging evaluation, and careful manipulation of the coil embolization resulted in a good outcome.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The author(s) confirms that there was no use of Artificial Intelligence (AI)-Assisted Technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Journal or its management. The information contained in this article should not be considered to be medical advice; patients should consult their own physicians for advice as to their specific medical needs.
Acknowledgments
We wish to thank Dr. Ryokichi Yagi, Dr. Fumihisa Kishi, Dr. Daiji Ogawa, and Dr. Keiichi Yamada for their advice on experimental design.
References
1. Crompton MR. The pathology of ruptured middle-cerebral aneurysms with special reference to the differences between the sexes. Lancet. 1962. 2: 421-5
2. Dong LW, Yamada K, Ohta T, Takahashi N. Ruptured intracranial aneurysm combined with multiple cerebral vessel anomalies; a case report. No Shinkei Geka. 1991. 19: 975-8
3. Eto A, Nakai K, Aikawa H, Iko M, Kouhei N, Kazekawa K. Unruptured cerebral aneurysm associated with fenestration of the anterior cerebral artery successfully treated with coil embolization using an intracranial stent: A case report. No Shinkei Geka. 2015. 43: 75-8
4. Fawcett E, Blachford JV. The circle of Willis: An examination of 700 specimens. J Anat Physiol. 1905. 40: 63.2-70
5. Inagawa T, Yamada T, Takeda T, Taguchi H. Aneurysms of the fenestrated anterior cerebral artery. Report of two cases. Neurol Med Chir (Tokyo). 1983. 23: 211-5
6. Iwabuchi N, Saito A, Fujimoto K, Nakamura T, Sasaki T. Unruptured saccular aneurysm arising from the fenestrated A1 segment of the anterior cerebral artery: Report of 2 cases. Case Rep Neurol. 2018. 10: 140-9
7. Komiyama M, Nakajima H, Nishikawa M, Yasui T. Middle cerebral artery variations: Duplicated and accessory arteries. AJNR Am J Neuroradiol. 1998. 19: 45-9
8. Mizoue T, Kiya K, Magaki T, Sakoguchi T, Kondo H, Miyoshi H. Anterior cerebral artery aneurysm related horizontal portion fenestration and accessory middle cerebral artery: Case report. J Neuroendovasc Ther. 2014. 8: 207-12
9. Ohshima K, Terada T, Hiyama T, Ookubo S, Ikeda R, Kobayashi H. Hemorrhagic complications of endovascular coil embolization for very small intracranial aneurysms. Surg Cereb Stroke. 2013. 41: 110-5
10. Ohta H, Kondoh H, Umemura T, Futatsuya K, Masaki H, Yamamoto J. Unruptured aneurysm arising from fenestrated anterior cerebral artery, associated with accessory anterior cerebral artery and accessory middle cerebral artery, with a quasi-moyamoya disease of neurofibromatosis Type 1: Case report. Jpn J Stroke. 2022. 44: 273-8
11. Padget DH. The development of the cranial arteries in the human embryo. Contribution to embryology. Carnegie Inst. 1948. 32: 205-61
12. Takahara M, Fukuda K, Kawano D, Yoshinaga S, Fukumoto H, Horio Y. Usefulness of adjunctive technique with a TACTICS catheter for coil embolization of cerebral aneurysms. J Neuroendovasc Ther. 2021. 15: 589-94
13. Terui K, Obayashi S, Shimizu M, Ozaki F, Moriwaki H, Ryujin Y. Unruptured aneurysm arising from fenestration of the horizontal (A1) segment in the anterior cerebral artery: A case report and review of the literature. No Shinkei Geka. 2010. 38: 545-50
14. Tsutsumi M, Aikawa H, Onizuka M, Iko M, Kodama T, Nii K. Coil embolization for tiny ruptured anterior communicating aneurysm. Surg Cereb Stroke. 2009. 37: 162-6
15. Yamaura I, Uramoto S, Kidera M, Matsumoto T, Fukushima Y, Shinko A. Coil embolization of small aneurysm with a maximum diameter of 3 mm. J Neuroendovasc Ther. 2010. 4: 99-105

