

- Spinal Unit (UVM), Department of Orthopaedics, Centro Hospitalar Universitário do Porto, Porto,
- Department of Orthopedics, Centro Hospitalar de Trásos-Montes e Alto Douro, Vila Real, Portugal,
- Instituto de Ciências Biomédicas Abel Salazar, Porto, Portugal.
Correspondence Address:
Ricardo Rodrigues-Pinto
Spinal Unit (UVM), Department of Orthopaedics, Centro Hospitalar Universitário do Porto, Porto,
Instituto de Ciências Biomédicas Abel Salazar, Porto, Portugal.
DOI:10.25259/SNI_761_2020
Copyright: © 2020 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Catarina Silva Pereira1, António Lemos Lopes2, Ricardo Rodrigues-Pinto1,3. Sequential traumatic cervical fractures after paragliding accidents – A case report and literature review. 10-Feb-2021;12:47
How to cite this URL: Catarina Silva Pereira1, António Lemos Lopes2, Ricardo Rodrigues-Pinto1,3. Sequential traumatic cervical fractures after paragliding accidents – A case report and literature review. 10-Feb-2021;12:47. Available from: https://surgicalneurologyint.com/surgicalint-articles/10585/
Date of Submission
25-Oct-2020
Date of Acceptance
15-Dec-2020
Date of Web Publication
10-Feb-2021
Abstract
Background: Sports related cervical spine trauma may range from minor injuries to severe life-threatening fractures with spinal cord injuries as following paragliding accidents.
Case Description: A 52-year-old male sustained C4-C5 and C6-C7 fracture-dislocations (American Spinal Injury Association-D) attributed to a paragliding accident. He underwent a C5 corpectomy with C4-C6 anterior fusion. Three years later, he again sustained a paragliding accident, now resulting in a C6-C7 fracture-dislocation that required a C6-C7 anterior discectomy fusion. However, when this latter fusion “failed” 1 month later, he subsequently required a 360° fusion performed as a two-stage procedure. Further, 2 years later, he was involved in a motor vehicle accident resulting in an odontoid fracture.
Conclusion: Unstable spinal fractures require surgical fixation to prevent neurological injury. Long cervical fusions create lever arms that increase the stress to adjacent levels, rendering them prone to future injury.
Keywords: Cervical fusion, Cervical spine fractures, Paragliding accidents, Spinal cord injuries
INTRODUCTION
About 2–4% of all trauma patients have cervical spine injuries (CSIs), and roughly 20% sustain spinal cord injuries. The most common causes of CSI are falls and motor vehicle accidents, followed by diving into shallow water, firearm injuries, and sport activities; paragliding accidents are exceedingly rare.[
CASE REPORT
A 52-year-old male sustained a CSI in a paragliding accident following which he exhibited bilateral weakness in the C6 root distribution without myelopathy (e.g., consistent with American Spinal Injury Association [ASIA] Impairment Scale of D). The cervical X-ray/MR/ computed tomography (CT) studies identified C4-C5 and C5-C6 fracture-dislocations warranting an emergent C5 corpectomy with anterior C4-C6 iliac crest strut fusion with plating [
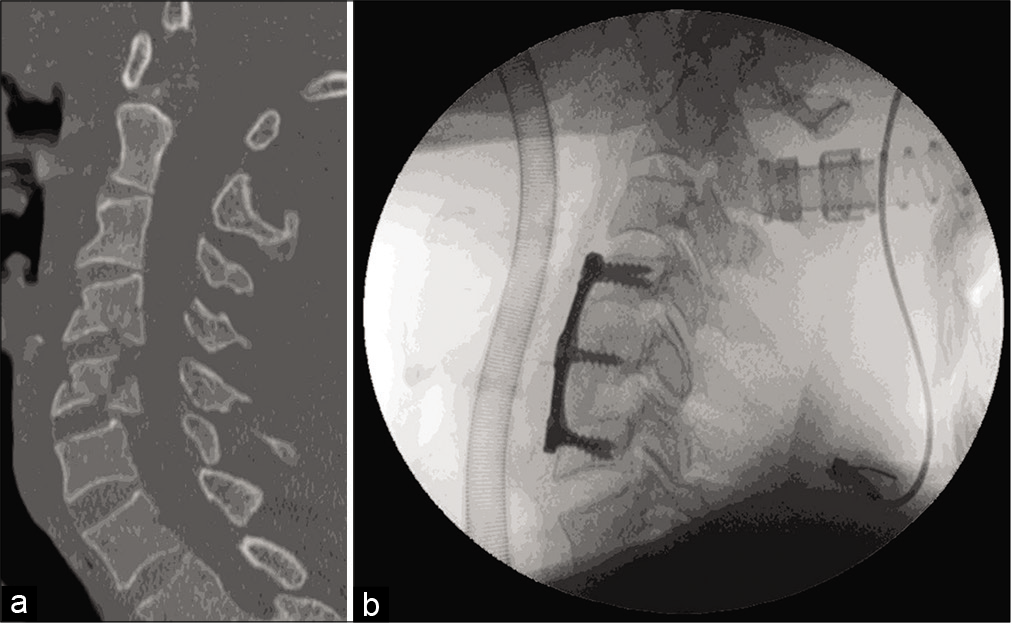
Figure 1:
(a) Cervical fracture-dislocation. Admission computed tomography scan, May 2011: sagittal views. “Fracture-dislocation of the C4 vertebra on the C5 vertebra and C5 vertebra on the C6 vertebra with retrolisthesis. Associated laminar fractures and subdislocation of the facet joints of C4-C5 and C5-C6 (b) Cervical fracture-dislocation. Fluoroscopic intraoperative lateral view: C5 corpectomy with anterior cervical fusion with iliac crest autograft (Badgley and Bailey) and C4-C6 plate.
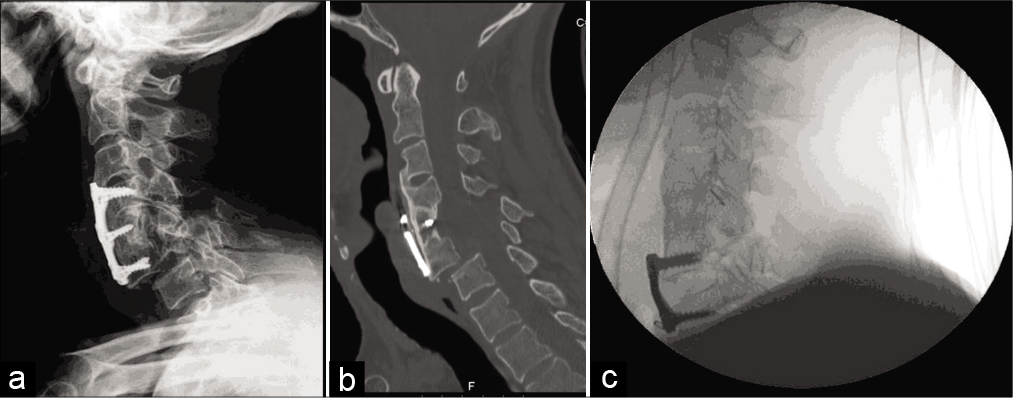
Figure 2:
(a) Admission X-ray after second paragliding accident, March 2014: lateral view C6-C7 dislocation. (b) Admission computed tomography scan after second paragliding accident, March 2014: lateral view C6-C7 dislocation. (c) Fluoroscopic intraoperative lateral view: C6-C7 anterior cervical discectomy and fusion with iliac crest autograft (Smith-Robinson) and C6-C7 plate.
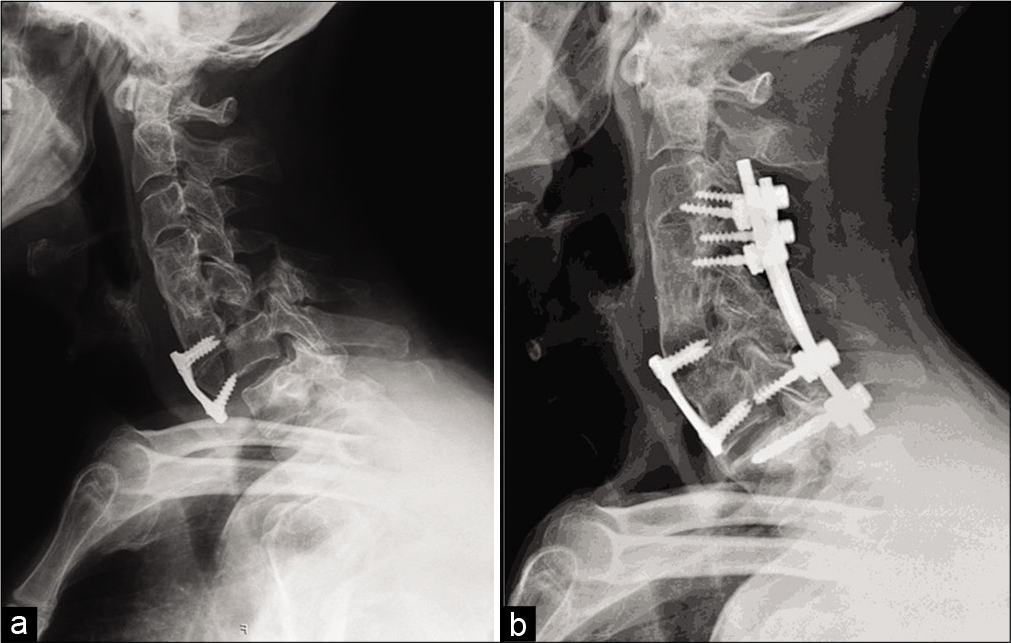
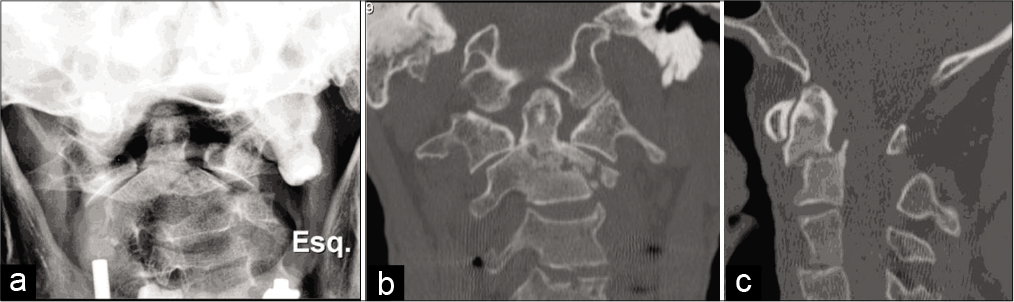
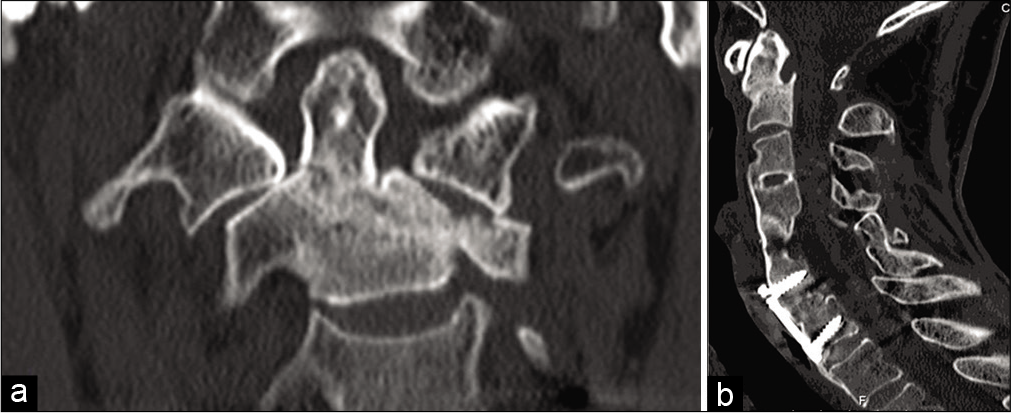
Figure 4:
(a) Admission X-ray (transoral view) and computed tomography (CT) scan. (b) June 2016: Anderson and D’Alonzo Type III odontoid fracture with the left lateral mass extension (CT scan, coronal view) (c) June 2016: Anderson and D’Alonzo Type III odontoid fracture with the left lateral mass extension (CT scan, sagittal view).
DISCUSSION
In this case report, the first paragliding accident caused a C4-C5 and a C5-C6 fracture-dislocation treated with a C5 corpectomy and C4-C6 strut/plated fusion. Two years later, the long lever arm increased the stress/susceptibility to the second paragliding accident resulting in a C6-C7 fracture requiring an ACDF.
When this second procedure failed within 1 postoperative month, the patient required an anterior C6-C7 revision plus a posterior C3-T1 fusion.
Here, the adjunctive posterior cervical fusion provided additional immediate stabilization and enhanced the probability of successful C6-C7 arthrodesis.[
CONCLUSION
This case highlights the importance of understanding the biomechanics behind cervical spine fusions and that long fusions may require posterior complementary spine stabilization. While the patient has been submitted to multiple surgical procedures he recovered fully from the initial neurological injury and shows complete union of his fractures
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Kruger-Franke M, Siebert CH, Pforringer W. Paragliding injuries. Br J Sports Med. 1991. 25: 98-101
2. Marcon RM, Cristante AF, Teixeira WJ, Narasaki DK, Oliveira RP, de Barros Filho TE. Fractures of the cervical spine. Clinics (Sao Paulo). 2013. 68: 1455-61
3. Sundstrom T, Asbjornsen H, Habiba S, Sunde GA, Wester K. Prehospital use of cervical collars in trauma patients: A critical review. J Neurotrauma. 2014. 31: 531-40
4. Vaccaro AR, Falatyn SP, Scuderi GJ, Eismont FJ, McGuire RA, Singh K. Early failure of long segment anterior cervical plate fixation. J Spinal Disord. 1998. 11: 410-5

