

- Department of Neurosurgery, University of Helsinki and Helsinki University Hospital, Helsinki, Finland
- Department of Neurosurgery, Barrow Neurological Institute, Phoenix, Arizona, USA
Correspondence Address:
Ahmad Hafez
Department of Neurosurgery, University of Helsinki and Helsinki University Hospital, Helsinki, Finland
DOI:10.4103/sni.sni_322_17
Copyright: © 2017 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Ahmad Hafez, Rahul Raj, Michael T. Lawton, Mika Niemelä. Simple training tricks for mastering and taming bypass procedures in neurosurgery. 06-Dec-2017;8:295
How to cite this URL: Ahmad Hafez, Rahul Raj, Michael T. Lawton, Mika Niemelä. Simple training tricks for mastering and taming bypass procedures in neurosurgery. 06-Dec-2017;8:295. Available from: http://surgicalneurologyint.com/?post_type=surgicalint_articles&p=8699
Date of Submission
31-Aug-2017
Date of Acceptance
06-Oct-2017
Date of Web Publication
06-Dec-2017
Abstract
Background:Neurosurgeons devoted to bypass neurosurgery or revascularization neurosurgery are becoming scarcer. From a practical point of view, “bypass neurosurgeons” are anastomosis makers, vessels technicians, and time-racing repairers of vessel walls. This requires understanding the key features and hidden tricks of bypass surgery. The goal of this paper is to provide simple and inexpensive tricks for taming the art of bypass neurosurgery. Most of these tricks and materials described can be borrowed, donated, or purchased inexpensively.
Methods:We performed a review of relevant training materials and recorded videos for training bypass procedures for 3 years between June 2014 and July 2017. In total, 1,300 training bypass procedures were performed, of which 200 procedures were chosen for this paper.
Results:A training laboratory bypass procedures is required to enable a neurosurgeon to develop the necessary skills. The important skills for training bypass procedures gained through meticulous practice to be as reflexes are coordination, speed, agility, flexibility, and reaction time. Bypassing requires synchronization between the surgeon's gross movements, fine motoric skills, and mental strength. The suturing rhythm must be timed in a brain–body–hand fashion.
Conclusion:Bypass-training is a critical part of neurosurgical training and not for a selected few. Diligent and meticulous training can enable every neurosurgeon to tame the art of bypass neurosurgery. This requires understanding the key features and hidden tricks of bypass surgery, as well as uncountable hours of training. In bypass neurosurgery, quality and time goes hand in hand.
Keywords: Bypass neurosurgery, simple training, skill
INTRODUCTION
Neurosurgery is considered to be a highly demanding field with time consuming and intensive training.[
Bypass procedures technically involve several phases such as preparing the donor vessel, harvesting a graft, preparing the recipient vessel, and microanastomosis. Training for bypass surgery consists of two main parts – eye-hand coordination and knowledge of microsuturing tricks. Eye-hand coordination enables fine motor skills and control of the microinstruments, which are the foundation of microsuturing.[
The goal of this paper is to provide simple and inexpensive tricks for taming the art of bypass neurosurgery. Most of these tricks and materials described can be borrowed, donated, or purchased inexpensively.
MATERIALS AND METHODS
We performed a review of relevant training materials and recorded videos for training bypass procedures performed by the first author (AH) for 3 years between June 2014 and July 2017. In total, 1,300 training bypass procedures were performed, of which 200 procedures were chosen for this paper. The 200 chosen procedures were all end-to-side procedures performed in 3 cm depth, simulating the most common superficial temporal artery to medial cerebral artery (STA-MCA) bypass procedure. Two types of materials were used: in 100, a 1-mm chicken wing vessel was used, and in 100, a 1-mm wet plastic tube was used. The recipient vessel was prepared the same way for all procedures [
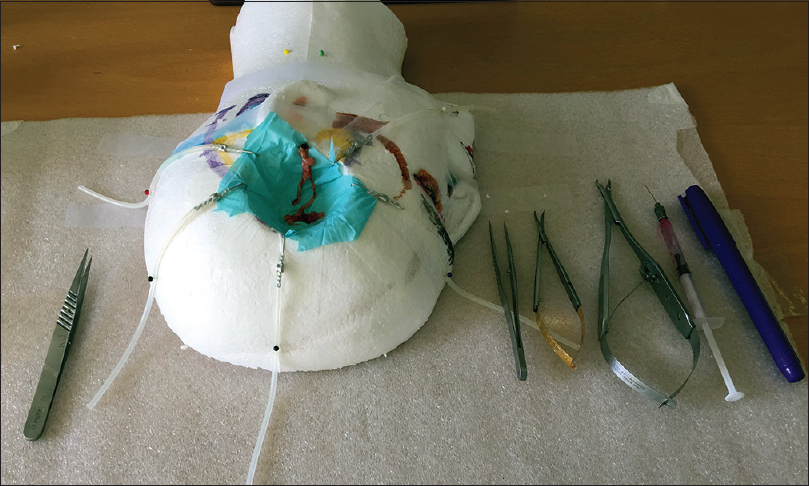
Figure 1
The bypass training setup and basic microtools. On the left side a pair of forceps, from the far right side a marker pen, a syringe, a clip holder, a pair of scissors, and a pair forceps. In the middle, a self-made model of a human head by Styrofoam. In the middle of the head (frontotemporal junction) and plastic tube vessel mimicking the superior temporal artery
RESULTS AND DISCUSSION
Phases of the micro-suture
The bypass neurosurgeon's goal is to develop the highest possible procedure velocity. For experienced bypass neurosurgeons, the warm-up stage is short, and may reach optimum velocity after a couple of sutures. Every microsuture consists of two major phases – the penetrating (support) phase and the knotting (recovery) phase. The neurosurgeon's speed is produced during both phases.
In the penetration phase, the needle driving hand applies gentle force against the wall of the vessel from a vertical orientation. Force is applied for a short time and the vessel wall is penetrated. To maintain flexible velocity, the neurosurgeon must be able to effectively apply suitable force during this short time period. After the penetration phase comes the knotting phase. The microsuture velocity is the product of these two phases. Further, our experience is that the two phases interact. If one phase gets slower the other will also slow down and vice versa.
Steps of the bypass procedure
Only three main instruments are needed in a majority of bypass procedures, two forceps and a scissor. Our experience and practicing in the lab supports self-handling of scissor by placing it as close as possible to the right hand of a right-handed neurosurgeon. The whole bypass procedure can be compared to a running performance. First comes the takeoff, followed by acceleration, and maintenance of maximum speed before decelerating and finishing the race (or bypass).
The takeoff phase at two points start (most time-consuming phase for most neurosurgeons) The acceleration phase The phase of maximum (constant speed) The deceleration phase (checking time). The finish.
During the takeoff phase the donor vessel is stitched to the recipient vessel at 12 and 6 o’clock. This requires a wide range of motion and different needle directions. This is often the most time-consuming phase. Following the takeoff phase, the acceleration phase starts with continuous repetition of stitches along the sides of the vessels. During the acceleration phase each stich should be placed faster and faster. After a few stitches, the surgeon reaches his/her maximum speed. When the stitches are coming to an end the surgeon usually has to decelerate to check the patency of the stitches before ending the suturing. Moving to the other side of the vessel should not disturb the procedure. In reality, the surgeon tends to move the chair, the microscope, the instruments, as we have the feeling of working in different sides of the “wall,” which is not true. For right-handed neurosurgeons, putting the upper endpoint stitch at 11 o’clock may be preferable and for left-handed neurosurgeons putting the upper endpoint stitch at 1 o’clock may be preferable.
For surgeons who perform uninterrupted stitching, we have found it preferable to tighten the thread after each stich instead of loosely suturing the whole vessel side and tightening the stitches at the end [
Skills needed for taming bypass procedures
Coordination: The skill of the neurosurgeon performing high-speeded movements requires nervous system control, which is the most critical aspect for effective bypassing.
Speed: This is obviously an important factor. Speed is tied to coordination, the ability to move the finger and hands at high velocities, and express precision and accuracy through those movements to proceed at high velocities.
Agility: The ability to change the hands and fingers position efficiently, which requires the integration of isolated small movement skills. It involves the combination of coordination, speed, reflexes, strength control, and stress endurance.
Flexibility: Bypass-mastering necessities high degree of flexibility in all parts of body, not only fingers and hands but also the whole upper-body, neck, and head.
Reaction time: “Nano” reaction time is a critical to perform a bypass in less than 20 minutes. Usually the time is lost after making the knot and getting a new grip of the needle.
These characteristics can be developed depending on the training program. The training program should be directed towards the development of all mentioned skills. A training laboratory giving the opportunity to train bypass procedures is required to enable the neurosurgeon to develop the skills necessary. Easily and cheaply available plastic tubes and chicken wings are suitable for training.
Bypass tricks
Below some tricks for the surgeon interested in bypass procedures:
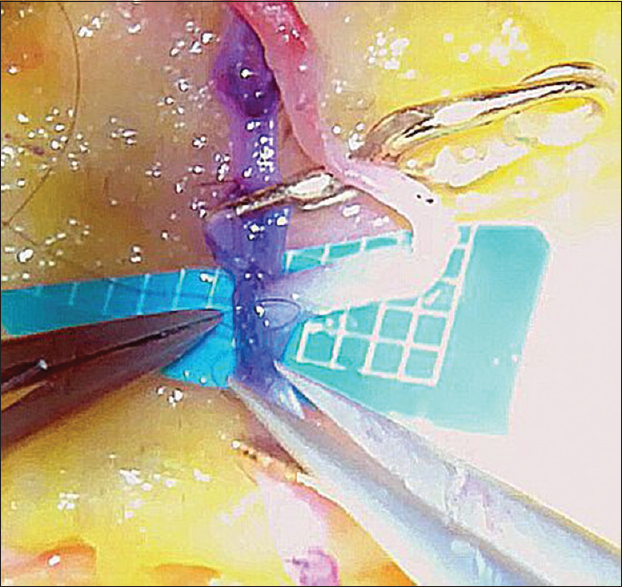
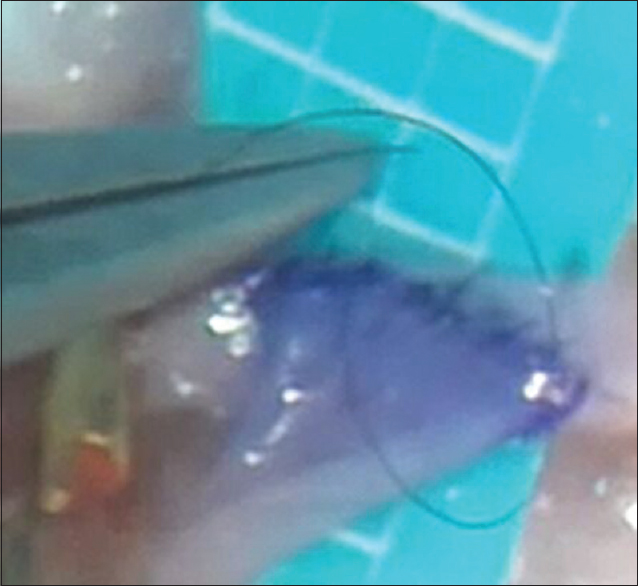
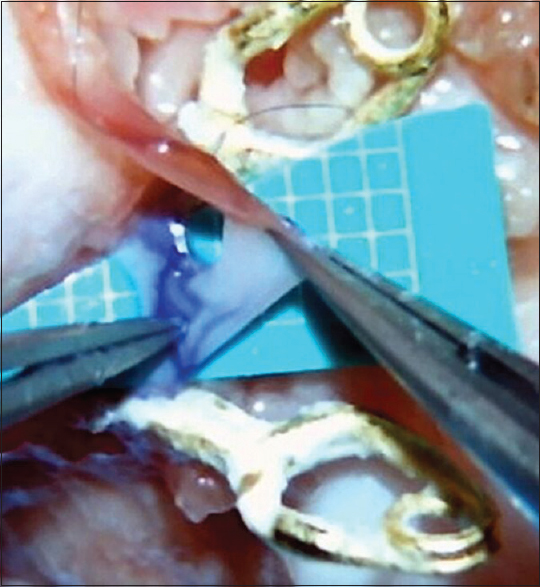
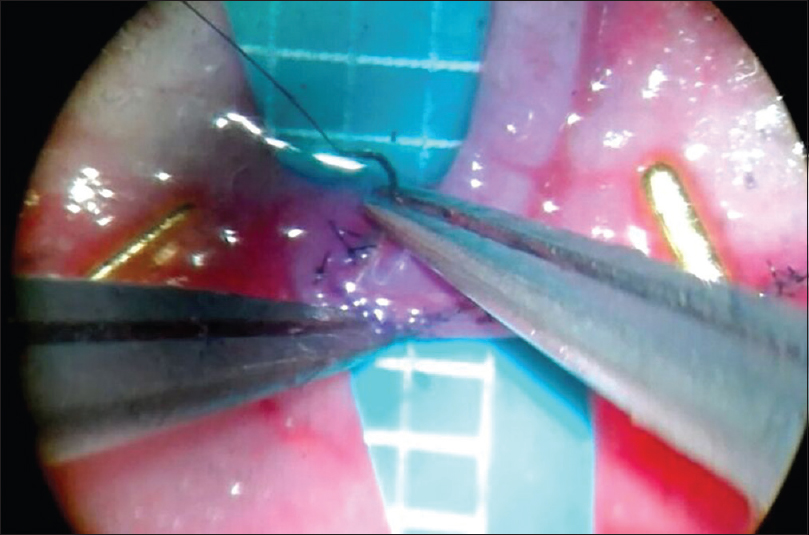
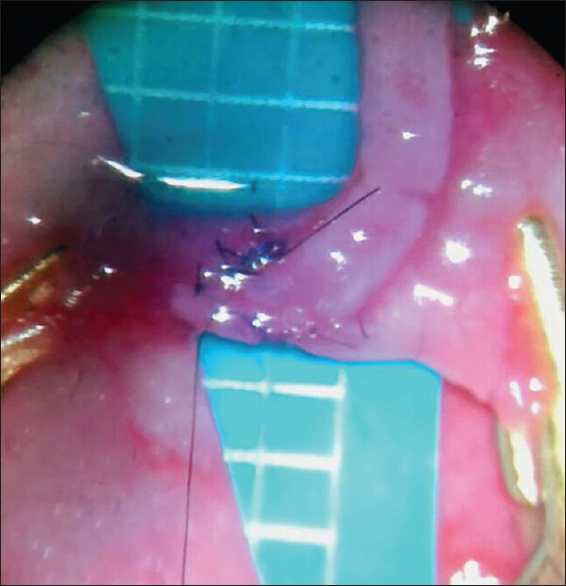
Hard sport may not be suitable the day of surgery. Fine tremor after vigorous sporting (e.g., weight lifting, boxing) may cause fine motor tremor several hours afterwards Prior to the operation, the neurosurgeon should avoid muscle exertion. For example, try to avoid straining yourself by holding the patient's head for prolonged times when placing the patient's head into the right position in the operation room Be relaxed and sit comfortably. Your favorite music may help you relax The position of the surgeon is important and should be coordinated with the microscope. The lens of the microscope should be vertical with the operation field. Thus, mild flexion of the neck is often required to optimize the surgeon's position. This combined with elbows gently squeezing against the waist to neutralize big joint movements gives you the optimal position for microsuturing Always keep the needle and the thread on a focused level in the microscope view The needle is held at a two-third distance from the tip Forceps should be leaner than the needle holder When making the knot, move only the forceps. Keep the needle holder still (unnecessary movement) Pull the first knot to your side, the second to the opposite, and the third again to you. When holding the end to cut the remainder of the thread, keep the thread between the grasp of the forceps. In this manner, the thread is under your control and it is easier to start the second knot [ Keep the angle between yourself and the suturing direction close to 180°. This allows you to put the suturing axis at 11–12 o’clock, or at 1 o’clock for left-handed neurosurgeons Putting the contralateral edge of the donor vessel inside the lumen of the recipient vessel is a practical trick to avoid penetrating the contralateral edge of the receiver [ A clean surgical field is important. Yet, exaggerated water flushing may move your needle and make you work under a water-blurred vision for some time [ Keep the end piece of the thread after penetrating the vessels as short as possible before starting the knot. This helps you find the thread's end piece quickly, saving a lot of unnecessary hand movements [
Training suggestions
Laying the foundation for eye-hand coordination and establish a microsuture routine. Perform microsutures for a minimum of 1 hour per day for at least 3 months. Use 7-0 or 8-0 thread. Do not focus on speed or time. The speed will be developed automatically Improve the microsuturing technique by clocking the time without placing too much emphasis on it. Use 9-0 thread. Putting a tube in the recipient vessel is suitable at this point. Continue with this stage for a minimum of 1 hour a day for 3 months Focus on avoiding unnecessary movements. Count the time of every second bypass performed for 3 months. Start video recording to identify unnecessary movements. Use 10-0 thread Perform bypasses with a ticking clock for every second. Focus on speed. Record bypasses and preferably have some “audience” looking at you. Work against the clock Continuous training. After you have mastered the basics of microsuturing maintaining the ability is of paramount importance. Train at least 1 hour two times a week continuously. In our experience, even 1 month of absence from microsuturing sets you back Several neurosurgeons go to the laboratory to rehearse microsuturing on the night before the actual surgery (or in the morning of the surgery).
CONCLUSION
Neurosurgical bypass surgery is the art of excellent eye-hand coordination, fine motor skills, and micro-suturing knowledge. Training without studying the principle and surgical details could lead to frustrating result. We have summarized the experience of experienced vascular neurosurgeons to provide practical tricks and tips in this paper. All points have been tested in the laboratory setting and in real surgery for an extended period of time. We believe that bypass-training is a critical part of neurosurgical training and not only for a selected few. Diligent and meticulous training can enable every neurosurgeon to tame the art of bypass neurosurgery.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Videos available on: www.surgicalneurologyint.com
References
1. Abla AA, Lawton MT. Revascularization for unclippable posterior inferior cerebellar artery aneurysms: Extracranial-intracranial or intracranial-intracranial bypass?. World Neurosurg. 2014. 82: 586-8
2. Aboud ET, Krisht AF, O’Keeffe T, Nader R, Hassan M, Stevens CM. Novel simulation for training trauma surgeons. J Trauma. 2011. 71: 1484-90
3. Alaraj A, Lemole MG, Finkle JH, Yudkowsky R, Wallace A, Luciano C. Virtual reality training in neurosurgery: Review of current status and future applications. Surg Neurol Int. 2012. 2: 52-
4. Chalouhi N, Zanaty M, Tjoumakaris S, Manasseh P, Hasan D, Bulsara KR. Preparedness of neurosurgery graduates for neuroendovascular fellowship: A national survey of fellowship programs. J Neurosurg. 2015. 123: 1113-9
5. Chowdhry SA, Spetzler RF. Genealogy of training in vascular neurosurgery. Neurosurgery. 2014. 74: S198-203
6. Eivazi S, Hafez A, Fuhl W, Afkari H, Kasneci E, Lehecka M. Optimal eye movement strategies: A comparison of neurosurgeons gaze patterns when using a surgical microscope. Acta Neurochir. 2017. 159: 959-66
7. Ezra DG, Aggarwal R, Michaelides M, Okhravi N, Verma S, Benjamin L. Skills acquisition and assessment after a microsurgical skills course for ophthalmology residents. Ophthalmology. 2009. 116: 257-62
8. Harada K, Morita A, Minakawa Y, Baek YM, Sora S, Sugita N. Assessing Microneurosurgical Skill with Medico-Engineering Technology. World Neurosurg. 2015. 84: 964-71
9. Harbaugh RE, Agarwal A. Training residents in endovascular neurosurgery. Neurosurgery. 2006. 59: S277-
10. Harnof S, Hadani M, Ziv A, Berkenstadt H. Simulation-based interpersonal communication skills training for neurosurgical residents. Israel Med Assoc J. 2013. 15: 489-92
11. Hooten KG, Lister JR, Lombard G, Lizdas DE, Lampotang S, Rajon DA. Mixed reality ventriculostomy simulation: Experience in neurosurgical residency. Neurosurgery. 2014. 10: 576-81
12. Korja M, Lehto H, Juvela S, Kaprio J. Incidence of subarachnoid hemorrhage is decreasing together with decreasing smoking rates. Neurology. 2016. 87: 1118-23
13. Liu JK, Kan P, Karwande SV, Couldwell WT. Conduits for cerebrovascular bypass and lessons learned from the cardiovascular experience. Neurosurg Focus. 2003. 14: e3-
14. Regelsberger J, Heese O, Horn P, Kirsch M, Eicker S, Sabel M. Training microneurosurgery-four years experiences with an in vivo model. Cent Eur Neurosurg. 2011. 72: 192-5
15. Russell SM, Post N, Jafar JJ. Revascularizing the upper basilar circulation with saphenous vein grafts: Operative technique and lessons learned. Surg Neurol. 2006. 66: 285-97
16. Sarkiss CA, Philemond S, Lee J, Sobotka S, Holloway TD, Moore M. Neurosurgical Skills Assessment: Measuring Technical Proficiency in Neurosurgery Residents through Intraoperative Video Evaluations. World Neurosurg. 2016. 89: 1-8
17. Schirmer CM, Mocco J, Elder JB. Evolving virtual reality simulation in neurosurgery. Neurosurgery. 2013. 73: 127-37
18. van der Zwan A. “How I Do It:” Non-occlusive High Flow Bypass Surgery. Acta Neurochir Suppl. 2014. 119: 71-6
19. Yadav YR, Parihar V, Ratre S, Kher Y, Iqbal M. Microneurosurgical Skills Training. J Neurol Surg. 2016. 77: 146-54

