

- Spinal Disorders Center, Fujieda Heisei Memorial Hospital, Fuijieda, Shizuoka, Japan,
- Department of Rehabilitation, Fujieda Heisei Memorial Hospital, Fuijieda, Shizuoka, Japan,
- Department of Neurosurgery, Gunma University Graduate School of Medicine, Maebashi, Gunma, Japan.
DOI:10.25259/SNI_438_2021
Copyright: © 2021 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Hiroya Shimauchi-Ohtaki1,3, Junya Hanakita1, Toshiyuki Takahashi1, Manabu Minami1, Ryo Kanematsu1, Naochika Sakaguchi2, Fumiaki Honda3. Small L4 ventral root schwannoma with acute onset of radicular pain: A case report. 21-Jun-2021;12:293
How to cite this URL: Hiroya Shimauchi-Ohtaki1,3, Junya Hanakita1, Toshiyuki Takahashi1, Manabu Minami1, Ryo Kanematsu1, Naochika Sakaguchi2, Fumiaki Honda3. Small L4 ventral root schwannoma with acute onset of radicular pain: A case report. 21-Jun-2021;12:293. Available from: https://surgicalneurologyint.com/surgicalint-articles/10904/
Date of Submission
01-May-2021
Date of Acceptance
25-May-2021
Date of Web Publication
21-Jun-2021
Abstract
Background: Patients with cauda equina schwannomas usually present with slowly progressive radiculopathy. Herein, we describe a 34-year-old male who presented with acute radiculopathy attributed to a small L4 ventral root schwannoma.
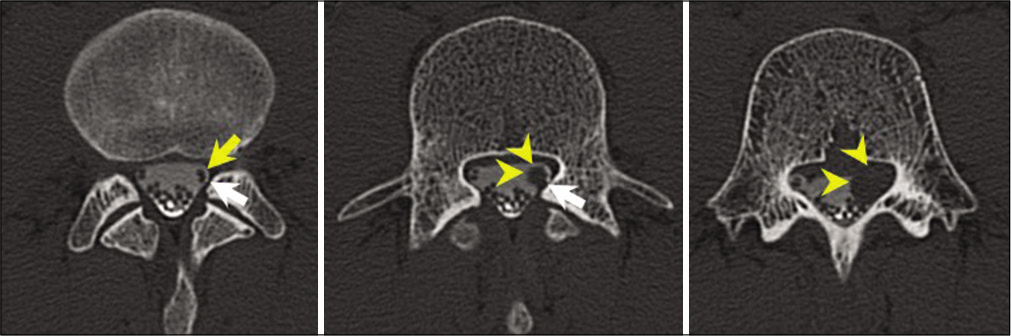
Case Description: A 34-year-old male suddenly developed left leg pain. Magnetic resonance imaging (with/without contrast) revealed a small intradural mass lesion involving the L4 nerve root that was enhanced with contrast (size: 9 × 12 × 12 mm). The computed tomography myelogram revealed that the tumor had originated from the L4 ventral root and compressed the dorsal root in the lateral recess. Following a decompressive laminectomy for tumor removal, the patient’s radicular pain improved. The histological diagnosis was consistent with a schwannoma.
Conclusion: Small cauda equina schwannomas involving ventral nerve roots can cause acute radiculopathy readily relieved with decompressive laminectomies for tumor excision.
Keywords: Acute radiculopathy, Cauda equine, Spinal schwannoma, Ventral root
INTRODUCTION
Spinal schwannomas are benign tumors that constitute 40–45% of all cauda equina tumors.[
CASE DESCRIPTION
History and examination
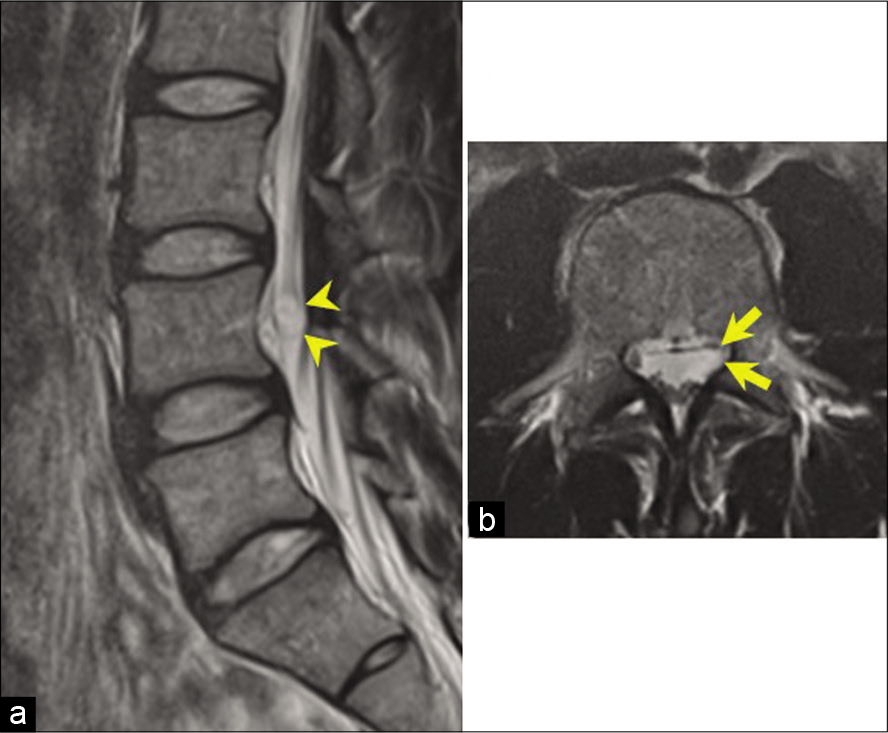
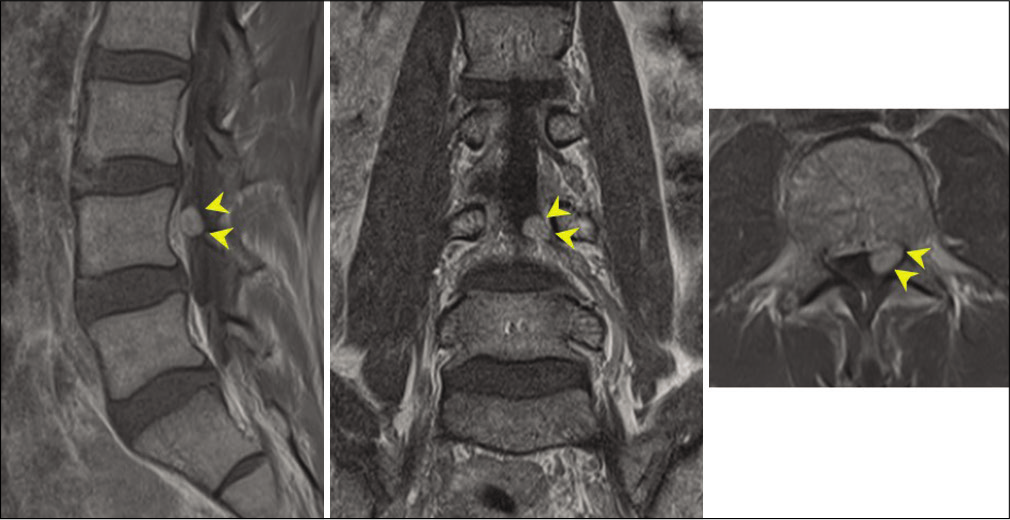
A 34-year-old male suddenly developed left lower extremity pain. The MRI with/without contrast revealed a small intradural extramedullary mass at the L4 level; the lesion was hypointense on T1-weighted images, hyperintense on T2-weighted images, and homogeneously enhanced with contrast (size: 9 × 12 × 12 mm, occupying 34% of the spinal canal in the axial view)[
Operative procedure
When a left L3-4 partial laminectomy was performed, the tumor was found to originate from the left L4 ventral root [
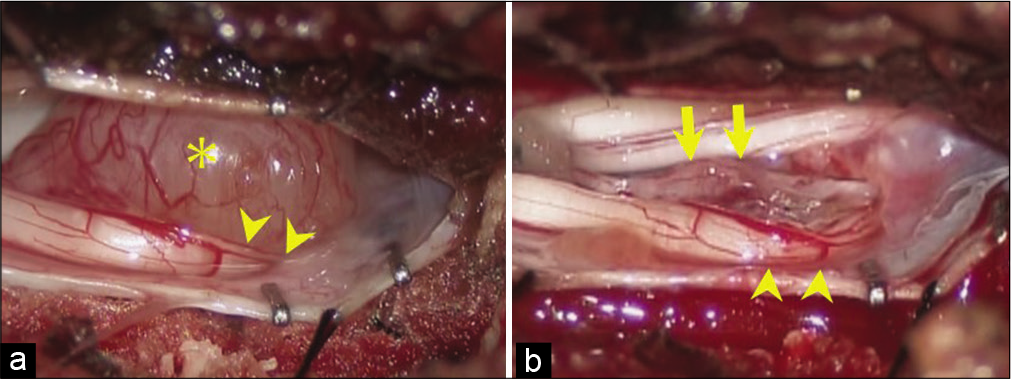
Figure 4:
Intraoperative photographs. (a) The tumor was observed after opening the dura and arachnoid membrane. The tumor (asterisk) markedly compressed the left L4 dorsal root (arrowheads). (b) Tumor resection achieved subtotal resection. The L4 dorsal root was released from the tumor compression. Arrows and arrowheads indicate the L4 ventral and dorsal nerve roots, respectively.
Histology
The postoperative histological diagnosis was consistent with a benign schwannoma (World Health Organization Grade I). The lesion was immunopositive for the S-100 protein, and the Ki-67 labeling index was 12.7% without evidence of necrosis or intratumoral hemorrhage.
Postoperative course
Within 3 weeks postoperatively, the L4 radicular pain improved from visual analog scale 8 to 3. Postoperative MRI confirmed a small residual tumor.
DISCUSSION
Acute neurological deficits associated with spinal schwannomas are rare.[
In the present case, the acute onset of pain and L4 radiculopathy were attributed to a small schwannoma originating from the L4 ventral nerve root. As the lesion filled the lateral recess, compressing both the L4 sensory and motor components, tumor excision was warranted.
Size correlating with onset of symptoms for cauda equina schwannomas
Cauda equina schwannomas are often larger than in the cervical or thoracic regions as there is more room within the lumbar spinal canal.[
MR findings for cauda equina schwannomas
Cauda equina schwannomas, like all schwannomas, typically appear hypointense on T1 and hyperintense on T2-weighted MR images.[
CONCLUSION
A cauda equina schwannoma arising from a ventral lumbar L4 nerve root resulted in acute pain/lumbar radiculopathy that was readily diagnosed with contrast-enhanced MRI/ myelo-CT and managed with tumor excision.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Cervoni L, Celli P, Scarpinati M, Cantore G. Neurinomas of the cauda equina clinical analysis of 40 surgical cases. Acta Neurochir (Wien). 1994. 127: 199-202
2. Fujii K, Sakane M, Abe T, Nakagawa T, Sakai S, Tatsumura M. Tumor occupation in the spinal canal and clinical symptoms of cauda equina schwannoma: An analysis of 22 cases. Asian Spine J. 2016. 10: 1079-84
3. Hanakita J, Suwa H, Nagayasu S, Nishi S, Iihara K, Sakaida H. Clinical features of intradural neurinomas in the cauda equina and around the conus medullaris. Neurochirurgia (Stuttg). 1992. 35: 145-9
4. Ichinose T, Takami T, Yamamoto N, Tsuyuguchi N, Ohata K. Intratumoral hemorrhage of spinal schwannoma of the cauda equina manifesting as acute paraparesis--case report. Neurol Med Chir (Tokyo). 2009. 49: 255-7
5. Jenkins AL III, Ahuja A, Oliff AH, Sobotka S. Spinal schwannoma presenting due to torsion and hemorrhage: Case report and review of literature. Spine J. 2015. 15: e1-4
6. Mahadewa T, Harsan H, Nugroho S, Bernstein M. Postoperative recovery of complete sudden paraplegia due to lumbar schwannoma. Case report. J Neurosurg Spine. 2005. 2: 601-3
7. Shrier DA, Rubio A, Numaguchi Y, Powers JM. Infarcted spinal schwannoma: an unusual MR finding. AJNR Am J Neuroradiol. 1996. 17: 1566-8

