

- Department of Neurosurgery, Advanced Neurology and Superspeciality Hospital, Jaipur, Rajasthan, India.
- Department of Neurosurgery, Shri Balaji Superspeciality Hospital, Raipur, Chhattisgarh, India.
Correspondence Address:
Sandeep Bhardwaj, Department of Neurosurgery, Advanced Neurology and Superspeciality Hospital, Jaipur, Rajasthan, India.
DOI:10.25259/SNI_1224_2021
Copyright: © 2022 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Sandeep Bhardwaj1, Manish Chaurasiya2, Sunit Shah1. Spontaneous cervicothoracic epidural misinterpreted as transient ischemic attack (TIA). 20-Jan-2022;13:19
How to cite this URL: Sandeep Bhardwaj1, Manish Chaurasiya2, Sunit Shah1. Spontaneous cervicothoracic epidural misinterpreted as transient ischemic attack (TIA). 20-Jan-2022;13:19. Available from: https://surgicalneurologyint.com/surgicalint-articles/11357/
Date of Submission
09-Dec-2021
Date of Acceptance
01-Jan-2022
Date of Web Publication
20-Jan-2022
Abstract
Background: The acute onset of a spontaneous spinal epidural hematoma (SSEH) is an uncommon cause of spinal cord compression. Early diagnosis and treatment are critical to avoid significant residual postoperative neurological deficits.
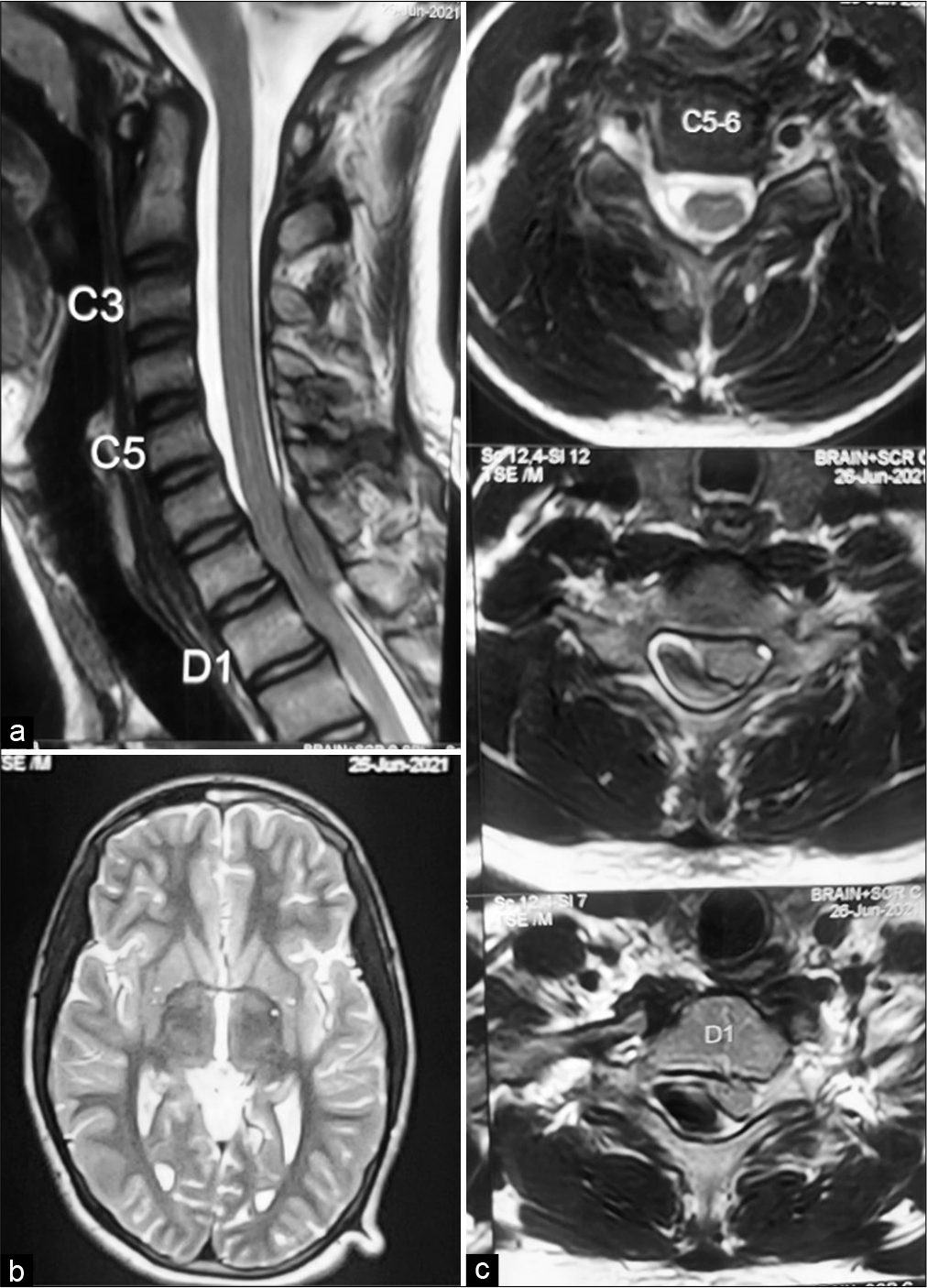
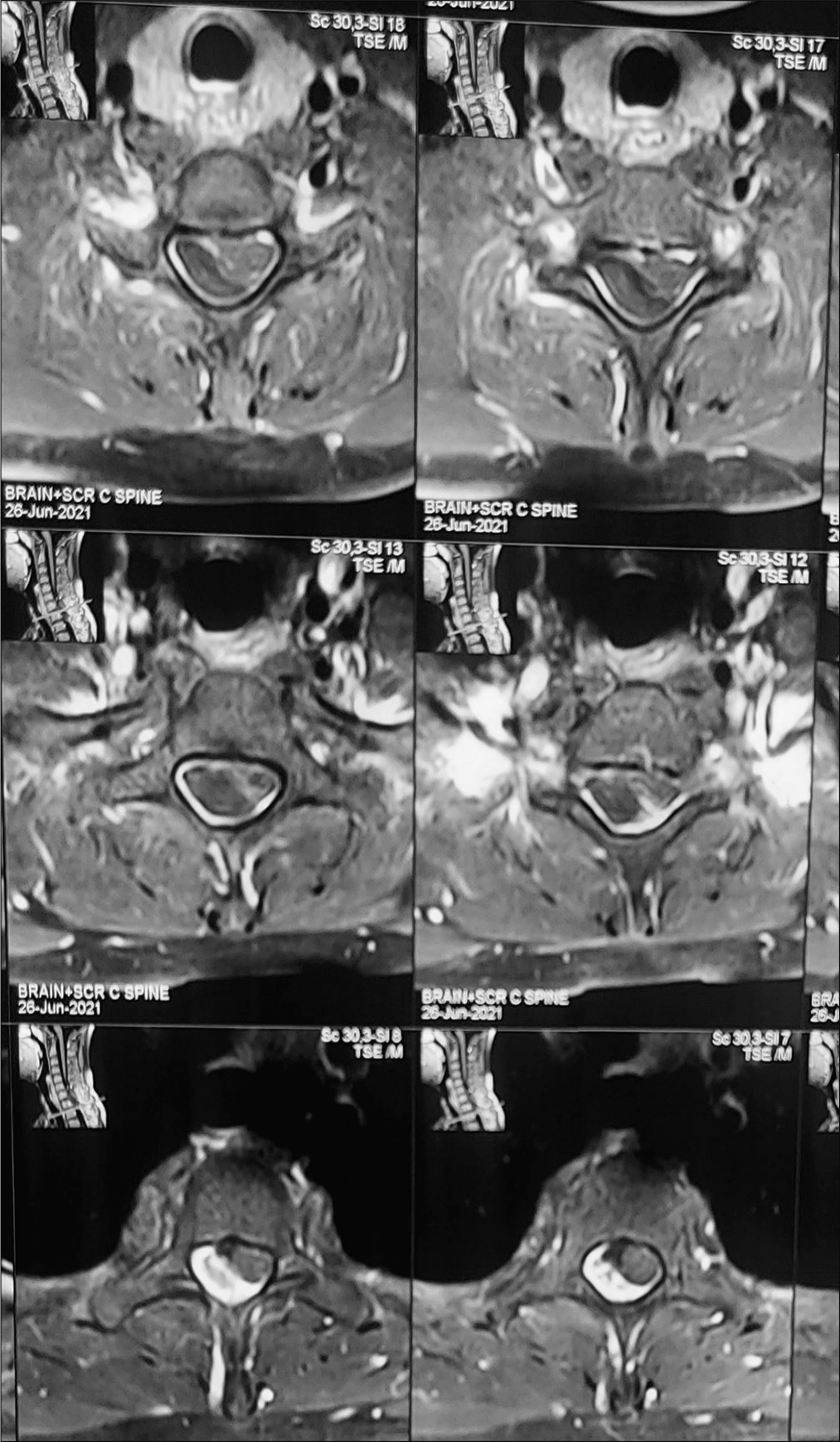
Case Description: A 15-year-old male presented with the sudden onset of a hemiparesis which recovered (4/5 weakness). The brain MR was negative, but spinal MRI revealed a dorsolateral extradural lesion extending from C7 to D1. At surgery, this proved to be a hematoma that we readily removed.
Conclusion: Spontaneous epidural hematomas are rare. They should be diagnosed promptly with MR, and typically warrant urgent/emergent surgical excision. Further, cases of SSEH resulting in hemiparesis may occasionally be misdiagnosed as attributed to a stroke or transient ischemic attack.
Keywords: Hemiparesis, Spontaneous hematoma, Transient ischemic attack
INTRODUCTION
Spontaneous spinal epidural hematomas (SSEHs) are rare and are usually attributed to; nontraumatic causes such as hemophilia, sneezing or lifting, neoplasms, arteriovenous malformation, hypertension, straining, or anticoagulants.[
CASE REPORT
A 15-year-old male presented with the sudden onset of a hemiparesis (i.e., left upper limb 4/5 and left lower limb 4/5). The laboratory work up was negative for any coagulation abnormalities; normal international normalized ratio, prothrombin time, activated partial thrombin time, and bleeding/clotting times. The brain MRI was normal, thus largely ruling out a stroke. However, the cervical MR showed a dorsolateral left-sided epidural hematoma extending from C7 to D1 causing severe cord compression. The lesion was hyperintense on T1, hyperintense with a hypointense band on T2 studies, but did not enhance with contrast [
DISCUSSION
Most SSEH occurs during activities such as sneezing, coughing, coitus, bending, and straining. They may be accompanied by the rapid onset of quadriparesis, paraparesis, or rarely, hemiparesis. MRI is the imaging modality of choice to diagnose SSEH. In first 24 h, epidural hematoma is isointense to cord on T1 images and is usually hyperintense or heterogeneous on T2 images; within 48 h, SSEH becomes hyperintense both T1 and T2 sequences. Few patients warrant conservative management and acute deterioration may result in permanent neurological sequelae. More typically, SSEH is spinal surgical emergencies requiring, with decompressive laminectomy and hematoma evacuation. Further early surgery results in the best prognoses (i.e., the “earlier the better”).[
CONCLUSION
SSEH is rare and required urgent/emergent diagnosis with MR and typically surgical management/decompression. Rarely, for patients who present with a hemiparesis, MR studies are required to rule out stroke.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Baek BS, Hur JW, Kwon KY, Lee HK. Spontaneous spinal epidural hematoma. J Korean Neurosurg Soc. 2008. 44: 40-2
2. Duffill J, Sparrow OC, Millar J, Barker CS. Can spontaneous spinal epidural haematoma be managed safely without operation? A report of four cases. J Neurol Neurosurg Psychiatry. 2000. 69: 816-9
3. Groen R. Non-operative treatment of spontaneous spinal epidural hematomas: A review of the literature and a comparison with operative cases. Acta Neurochir (Wien). 2004. 146: 103-10
4. Kim KT, Cho DC, Ahn SW, Kang SH. Epidural hematoma related with low-dose aspirin: Complete recovery without surgical treatment. J Korean Neurosurg Soc. 2012. 51: 308-11
5. Zhong W, Chen H, You C, Li J, Liu Y, Huang S. Spontaneous spinal epidural hematoma. J Clin Neurosci. 2011. 18: 1490-4

