

- Department of Trauma and Emergency, All India Institute of Medical Science, Bhubaneswar, Odisha, India
- Department of Neurosurgery, All India Institute of Medical Science, Bhubaneswar, Odisha, India
- Department of ENT, All India Institute of Medical Science, Bhubaneswar, Odisha, India
Correspondence Address:
Ashis Patnaik
Department of ENT, All India Institute of Medical Science, Bhubaneswar, Odisha, India
DOI:10.4103/2152-7806.180466
Copyright: © Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Patnaik A, Mahapatra AK, Sarkar S, Samal DK. Spontaneous leaking craniopharyngioma causing preoperative chemical meningitis. Surg Neurol Int 14-Apr-2016;7:41
How to cite this URL: Patnaik A, Mahapatra AK, Sarkar S, Samal DK. Spontaneous leaking craniopharyngioma causing preoperative chemical meningitis. Surg Neurol Int 14-Apr-2016;7:41. Available from: http://surgicalneurologyint.com/surgicalint_articles/spontaneous-leaking-craniopharyngioma-causing-preoperative-chemical-meningitis/
Sir,
Spontaneous chemical meningitis in craniopharyngioma is a rare phenomenon. The cause of this meningitis is due to rupture of craniopharyngioma and release of chemical contents particularly cholesterol crystals. We report an interesting case of chemical meningitis due to a leaking craniopharyngioma rather than a ruptured one. Very few cases of leaking craniopharyngioma have been reported in the literature.[
A 13-year-old girl presented with an intermittent headache for last 1 year. She had complete loss of vision on the left side eye and progressively diminishing vision on the right one. The computed tomography (CT) scan showed a hypodense lesion in pituitary fossa with extension to the suprasellar region. There were areas of calcifications on the peripheral part of the lesion [
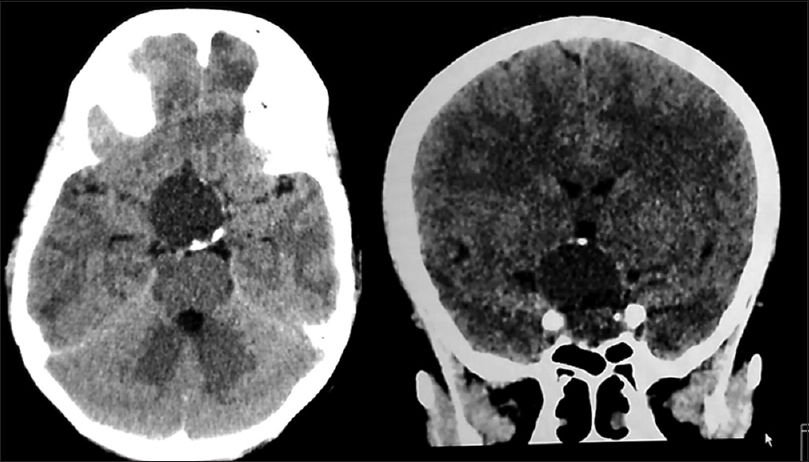
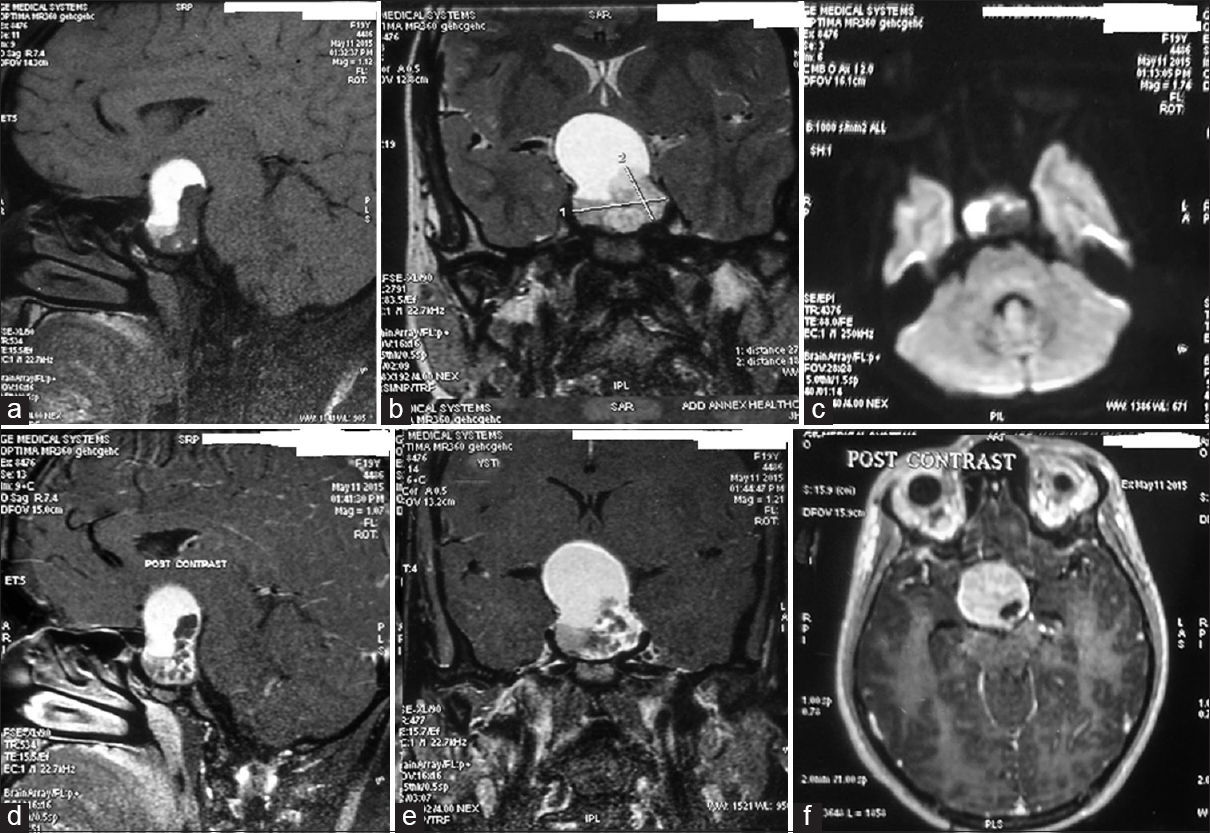
Figure 2
Magnetic resonance imaging pictures of the lesion. (a) T1-weighted sagittal image showing the lesion containing fat containing T1 hyperintense antero-superior and hypointense solid part in postero-inferior part. (b) T2-weighted coronal image of the lesion. (c) Diffusion image showing the solid part predominantly on left side. (d-f) Contrast images show the lesion to be minimally patchy enhancing
Aseptic or chemical meningitis is a rare complication in craniopharyngiomas particularly cystic ones, due to rupture and spillage of its contents containing cholesterol into the subarachnoid space, secreted by its squamous epilthelial lining. The occurrence of meningitis following rupture of the cyst is directly related to the cholesterol contents as its absence makes the rupture asymptomatic. Takahashi et al.,[
Suprasellar cystic tumors such as craniopharyngioma, dermoid, and epidermoid, Rathke's cleft cyst can rupture spontaneously with remission of symptoms particularly those caused by a compressive effect like vision symptoms. Cerebral infarction due to vasospasm following craniopharyngioma cyst rupture has also been reported in the literature.[
Our case was exclusive in that the meningitis episode occurred preoperatively without any reduction in the cyst size raising possibility of a bacterial cause. However, the CSF study established the chemical nature of the lesion. Neurosurgeons should be aware of such spontaneous leakage or rupture of the cyst in preoperative stage causing chemical meningitis in a cystic tumor. CSF and radiological examination must be done to establish the exact cause. Treatment is directed toward immediate management of meningitis followed by removal of the cause.
Financial Support and Sponsorship
Nil.
Conflicts of Interest
There are no conflicts of interest.
References
1. Hadden D, Allen I. Chemical meningitis due to rupture of a craniopharyngioma cyst. J R Soc Med. 2004. 97: 585-6
2. Krueger DW, Larson EB. Recurrent fever of unknown origin, coma, and meningismus due to a leaking craniopharyngioma. Am J Med. 1988. 84: 543-5
3. Kumar A, Kasliwal MK, Suri A, Sharma BS. Spontaneous asymptomatic rupture of cystic craniopharyngioma in a child: Case report and review of the literature. J Child Neurol. 2010. 25: 1555-8
4. Okamoto H, Harada K, Uozumi T, Goishi J. Spontaneous rupture of a craniopharyngioma cyst. Surg Neurol. 1985. 24: 507-10
5. Rajput D, Srivastva A, Kumar R, Mahapatra A. Recurrent chemical meningitis in craniopharyngioma without reduction in size of cyst: Case report of two cases and review of the literature. Turk Neurosurg. 2012. 22: 233-6
6. Satoh H, Uozumi T, Arita K, Kurisu K, Hotta T, Kiya K. Spontaneous rupture of craniopharyngioma cysts. A report of five cases and review of the literature. Surg Neurol. 1993. 40: 414-9
7. Shida N, Nakasato N, Mizoi K, Kanaki M, Yoshimoto T. Symptomatic vessel narrowing caused by spontaneous rupture of craniopharyngioma cyst – Case report. Neurol Med Chir (Tokyo). 1998. 38: 666-8
8. Takahashi T, Kudo K, Ito S, Suzuki S. Spontaneously ruptured craniopharyngioma cyst without meningitic symptoms – Two case reports. Neurol Med Chir (Tokyo). 2003. 43: 150-2
9. Tokiwa K, Nakayama K, Miyasaka Y, Matsumori K, Beppu T, Asao T. Cystic craniopharyngioma with spontaneous shrinkage of the cyst. Case report. Neurol Med Chir (Tokyo). 1984. 24: 954-7

