

- Department of Neurosurgery, Junshin Hospital, Kakogawa, Japan.
- Department of Neurosurgery, Kobe University Graduate School of Medicine, Kobe, Japan.
Correspondence Address:
Satoshi Inoue, Department of Neurosurgery, Junshin Hospital, Kakogawa, Japan.
DOI:10.25259/SNI_974_2023
Copyright: © 2024 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Satoshi Inoue1, Atsushi Fujita2, Eiji Kurihara1, Takashi Sasayama2. Steerable microcatheter for distal access of a giant cavernous carotid artery aneurysm during treatment with Pipeline Embolization Device: A case report and review of the literature. 09-Feb-2024;15:40
How to cite this URL: Satoshi Inoue1, Atsushi Fujita2, Eiji Kurihara1, Takashi Sasayama2. Steerable microcatheter for distal access of a giant cavernous carotid artery aneurysm during treatment with Pipeline Embolization Device: A case report and review of the literature. 09-Feb-2024;15:40. Available from: https://surgicalneurologyint.com/?post_type=surgicalint_articles&p=12735
Date of Submission
04-Dec-2023
Date of Acceptance
11-Jan-2024
Date of Web Publication
09-Feb-2024
Abstract
Background: In the treatment of giant cerebral aneurysms with flow-diverting stents, access to the distal parent artery is critical but occasionally challenging. This article provides our experience with a novel steerable microcatheter in such a situation, as well as a review of the literature.
Case Description: A 73-year-old woman presented with right ptosis and external ophthalmoplegia. Magnetic resonance angiography revealed a giant right cavernous internal carotid artery aneurysm. Endovascular treatment was planned with flow diversion, but distal access was not possible using the standard technique. A 2.4-Fr steerable microcatheter, Leonis Mova Selective, was implemented, and by bending the catheter tip toward the distal parent artery, a guidewire could be guided distally. After the catheter exchange, two flow-diverting stents were deployed successfully.
Conclusion: Steerable microcatheters may provide an option in treatment with flow-diverting stents for giant cerebral aneurysms where access to the distal parent artery is compromised.
Keywords: Buddy-wire technique, Complication, Flow diverter, Intra-aneurysmal looping, Stent retriever
INTRODUCTION
In the treatment of giant cerebral aneurysms with flow-diverting stents, access to the distal parent artery is critical but occasionally challenging.[
Leonis Mova (Sumitomo Bakelite, Tokyo, Japan) is a novel steerable microcatheter that received approval in Japan in November 2022 for its use in the head and neck region. The angle of the tip can be changed by manipulating the handle and can be fixed at an optimal angle. In the present case, we used the Leonis Mova to access the distal parent artery of a giant cavernous internal carotid artery (ICA) aneurysm that could not be accessed using standard techniques and successfully treated it with a flow diverter.
This report describes the technical aspects of the use of a steerable microcatheter for giant cerebral aneurysms. In addition, an initial review of the literature on the clinical use of steerable microcatheters for intracranial vessels is presented. To the best of our knowledge, only three giant cerebral aneurysms have been treated with steerable microcatheters.
CASE PRESENTATION
A 73-year-old woman developed ptosis and external ophthalmoplegia of the right eye. Magnetic resonance angiography showed a giant right cavernous ICA aneurysm and endovascular treatment with flow diversion was planned. The patient was started on aspirin and clopidogrel one month before treatment.
Endovascular treatment
Under general anesthesia and after general heparinization, a 6-Fr guiding sheath (Fubuki Dilator Kit, 80 cm; Asahi Intecc, Aichi, Japan) was placed from the right femoral artery into the right cervical ICA. The aneurysm originated from the C4 portion of the right ICA, and the diameter of the dome was 27.6 × 25.1 mm [
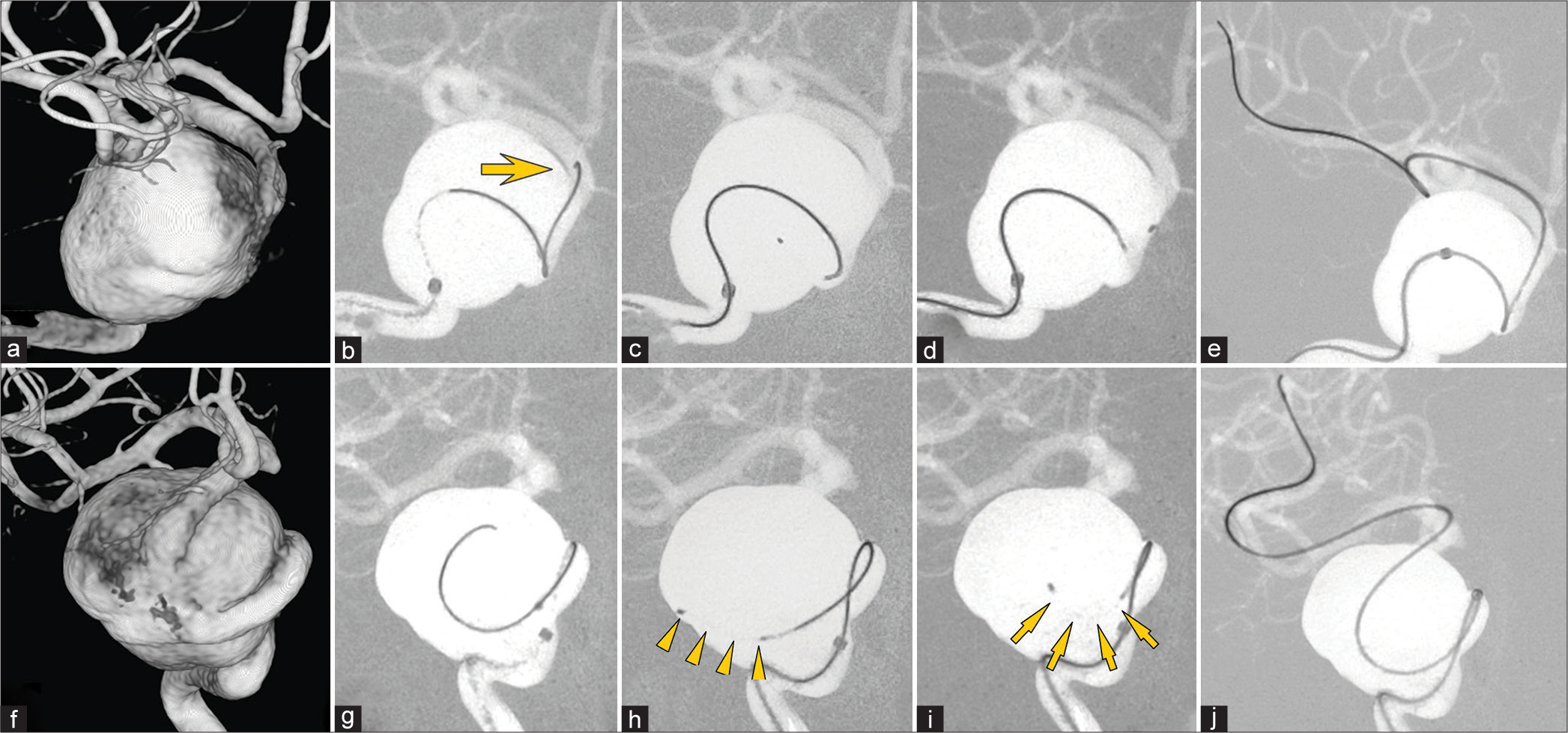
Figure 1:
(a and f) Three-dimensional rotational angiography shows a giant right cavernous internal carotid artery aneurysm (27 × 26 mm). (b and g) A regular 0.017-inch microcatheter and 0.014-inch guidewire (arrow) can not be guided into the distal parent artery. (c and h) The neutral position of the Leonis Mova Selective (arrowheads). (d and i) By bending the tip of the Leonis Mova Selective toward the distal parent artery (arrows), the guidewire can be guided into the middle cerebral artery (e and j).
Using a 5-Fr Navien, 115 cm (Medtronic, Minneapolis, MN, USA) as an intermediate catheter, we attempted to guide a Phenom 27 (Medtronic) and Chikai 14, 200 cm (Asahi Intecc) into the distal parent artery using the standard technique. However, although the guidewire could be guided to the origin of the distal parent artery, it could not be guided further distally [
The Leonis Mova was exchanged for a Phenom 27 using a Chikai 14, 300 cm (Asahi Intecc). During this procedure, the tip of the Phenom 27 was stuck at the orifice of the distal parent artery due to the “ledge effect” and could not be guided [
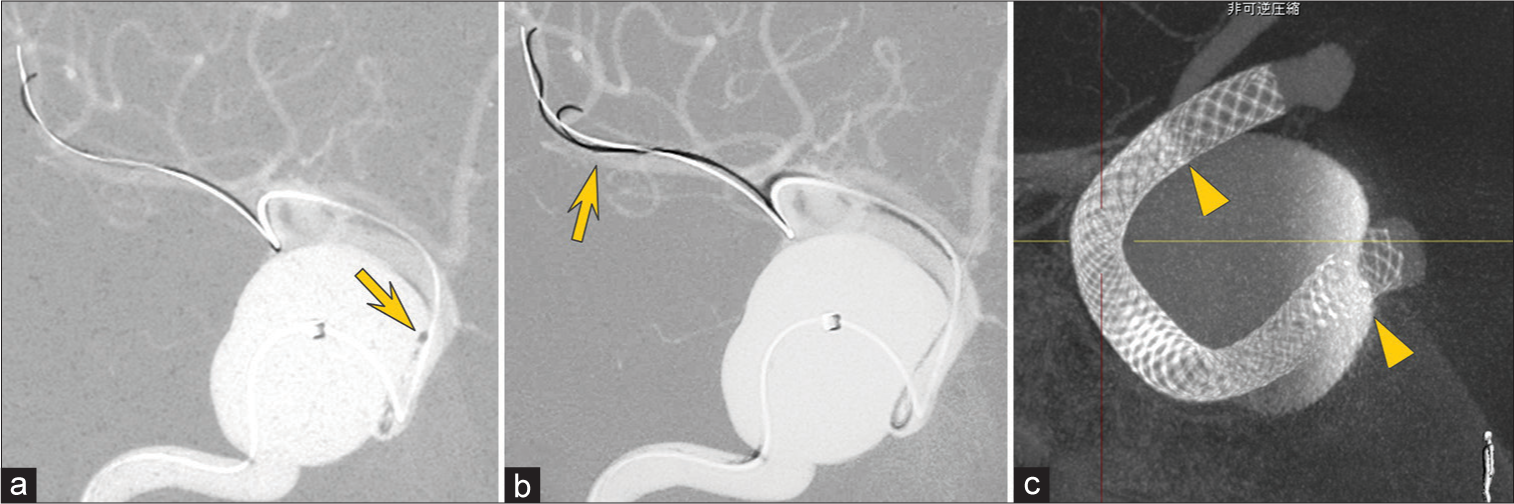
Figure 2:
(a) When exchanging the Leonis Mova Selective for a 0.027-inch microcatheter using a 0.014-inch, 300-cm guidewire, the tip of the latter catheter (arrow) interferes with the orifice and cannot be advanced into the parent artery. (b) By introducing a 0.010-inch guidewire in parallel, the catheter can be guided to the distal parent artery. (c) Two flow diverters are implanted (arrowheads indicate the second stent).
The postoperative course was good, and the patient’s ptosis began to improve on postoperative day 3. She was discharged on postoperative day 12.
DISCUSSION
Experience with Leonis Mova in giant cerebral aneurysms
In giant cerebral aneurysms, access to the distal parent artery can be difficult due to the unfavorable anatomy of the aneurysm, the acute branching angle of the parent artery, and the narrowing of the parent artery.[
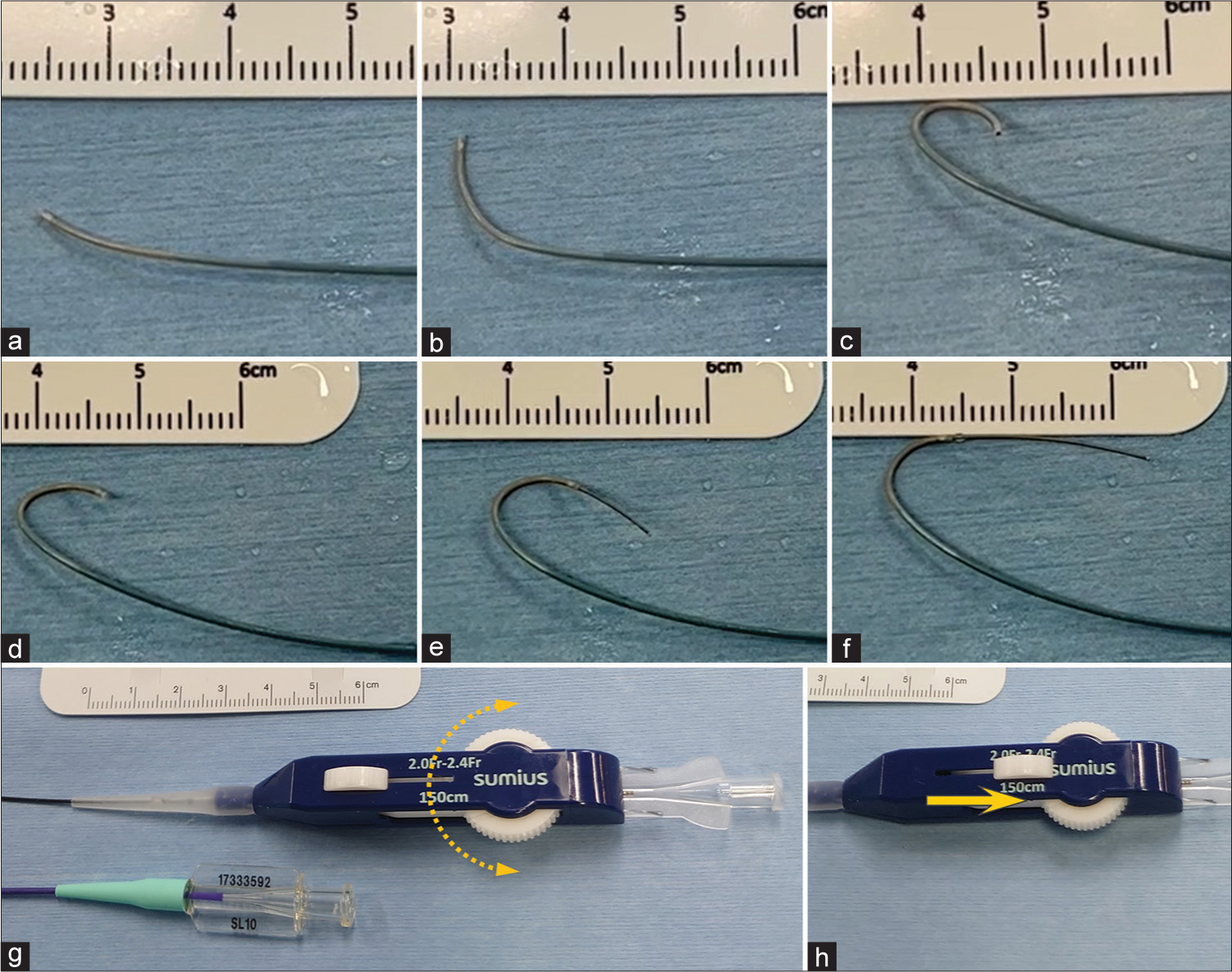
Figure 3:
(a-c) The Leonis Mova Selective can be bent at the tip and locked in shape at any angle by manipulating the handle. (d-f) Compared to without a 0.014-inch guidewire, the catheter tip shape is maintained when the wire is advanced 1 cm and 2 cm. (g and h) The control unit is larger than that of a regular microcatheter. By rotating the dial, the catheter tip can be bent in both directions (dashed arrow), and it is fixed by pulling the stopper (arrow).
To direct the catheter tip toward the parent artery orifice, it was necessary to rotate the Leonis Mova three-dimensionally, but the catheter did not have high torque transferability of its own. By rotating the Leonis Mova and guidewire while pulling them proximally as a single unit, the system was easily rotated. In addition, the aneurysm wall was used to limit the plane of movement of the catheter tip, making it easier to direct the tip toward the arterial orifice.
It is not recommended to bend the tip of the Leonis Mova with the guidewire in the tip; it is preferable to pull the guidewire back proximally before bending it. Except for the tip marker, the catheter tip is not highly visible. Therefore, the shape of the bent tip had to be estimated from the movement and direction of the tip marker, but this did not interfere with its actual use.
Review of previous reports on the use of steerable microcatheters for intracranial vessels
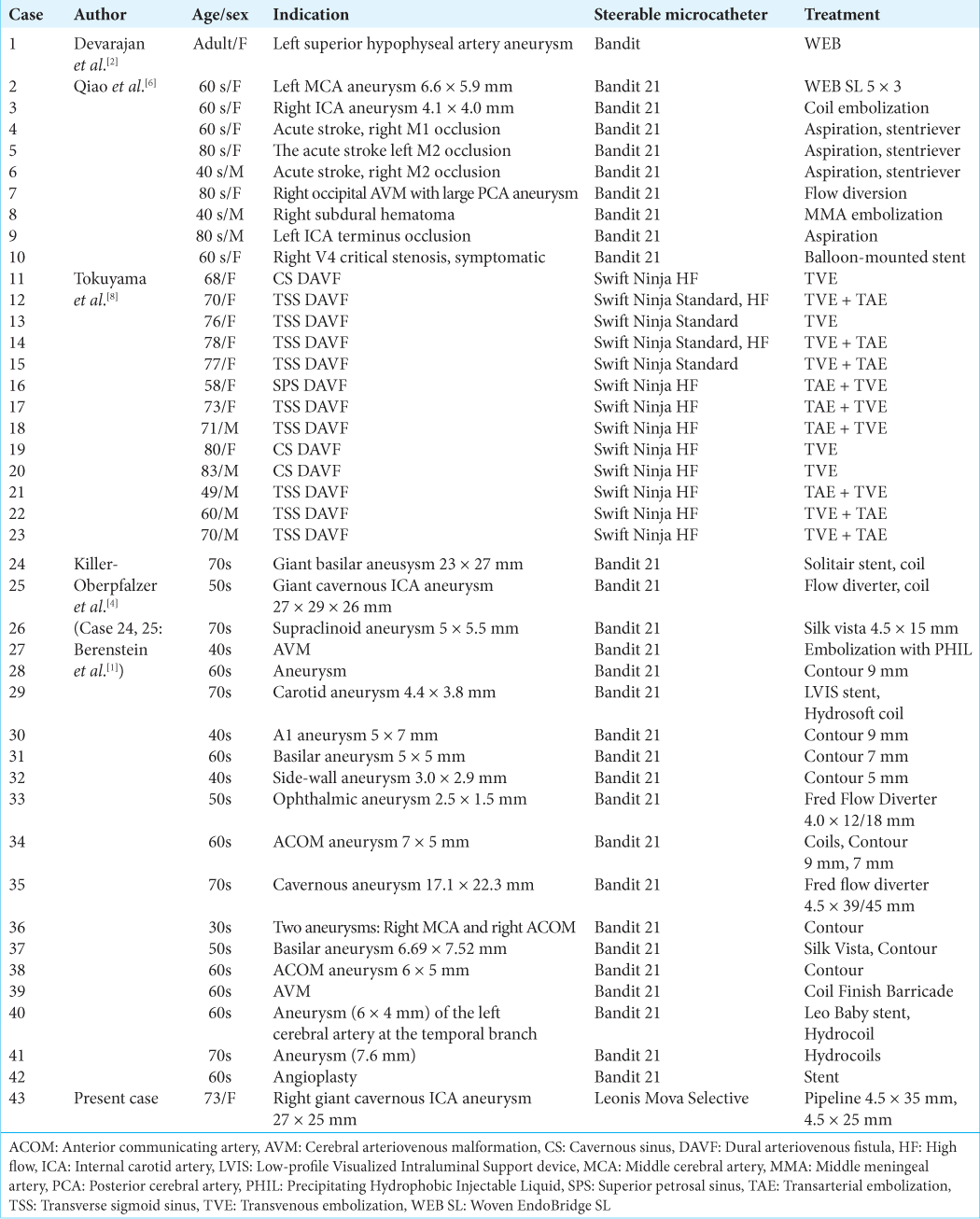
We searched PubMed using the keyword “steerable microcatheter” and found 57 reports. Among these were five reports of 42 cases using steerable microcatheters in the endovascular treatment of human intracranial vessels [
Access to the distal parent artery of giant cerebral aneurysms
Catheters for flow diverter deployment are relatively rigid, which limits their maneuverability. Therefore, if access to the distal parent artery is difficult, a catheter with a lower profile and higher maneuverability is first guided distally and then exchanged for a catheter designed for the flow diverter. However, catheter exchange carries the risk of vascular injury, distal wire perforation, and subarachnoid hemorrhage.[
If access to the distal parent artery is still difficult, the guidewire and microcatheter can be looped within the aneurysm and guided to the distal parent vessel, after which the loop in the aneurysm is removed.[
In the present case, the Leonis Mova was guided directly into the distal parent artery without looping within the aneurysm and then exchanged for a catheter for the flow diverter. To reduce the risk during the catheter exchange maneuver, we attempted to introduce the intermediate catheter into the distal parent artery, but this was not possible due to the tortuosity of the proximal parent artery. Considering the stress on the aneurysm wall and distal artery, as well as maneuverability, we used the smaller-diameter Leonis Mova. Although larger-diameter devices are available, the safety of direct deployment of flow-diverting stents with the Leonis Mova has not yet been established.
Buddy-wire technique
Another problem in directing larger-diameter, stiffer catheters for flow diverter deployment is the “ledge effect,” whereby the catheter tip snags at the distal parent artery orifice, preventing device navigation and potentially leading to serious complications due to unexpected device advancement. To avoid this, the “buddy-wire technique” has been reported, whereby the catheter is guided along two guidewires.[
CONCLUSION
Steerable microcatheters may provide an option in the deployment of flow-diverting stents for giant cerebral aneurysms where access to the distal parent artery is compromised.
Ethical approval
The research/study approved by the Institutional Review Board at Junshin Hospital, number 2023-006, dated 2023/12/05.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of Interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Journal or its management. The information contained in this article should not be considered to be medical advice; patients should consult their own physicians for advice as to their specific medical needs.
References
1. Berenstein A, Chapot R, Orion D, Barr JD, Cabiri O, Killer-Oberpfalzer M. Clinical and simulated experiences with the bendit articulating/steerable microcatheter in endovascular treatment: 2-dimensional operative video. Oper Neurosurg (Hagerstown). 2023. 25: e36-7
2. Devarajan A, Al-Kawaz M, Giovanni B, Tabani H, Shigematsu T, Fifi JT. Placement of an intrasaccular flow diverter in an intracranial sidewall aneurysm using the Bendit articulating microcatheter. J Neurointerv Surg. 2023. p. Online ahead of print
3. Dobrocky T, Lee H, Nicholson P, Agid R, Lynch J, Swaminathan SK. When two is better than one: The buddy-wire technique in flow-diversion procedures. Clin Neuroradiol. 2022. 32: 491-8
4. Killer-Oberpfalzer M, Chapot R, Orion D, Barr JD, Cabiri O, Berenstein A. Clinical experience with the Bendit steerable microcatheter: A new paradigm for endovascular treatment. J Neurointerv Surg. 2023. 15: 771-5
5. Lagios K, Mantatzis M. Vacuum for straightening the microcatheter after intra-aneurysmal looping: The “Lagman vacuum” technique. Interv Neuroradiol. 2019. 25: 438-41
6. Qiao Y, Zhang YJ, Tsappidi S, Mehta TI, Hui FK, editors. Initial clinical experience with the Bendit steerable articulating tip microcatheter for intracranial access and intervention. Interv Neuroradiol. 2023. p. Online ahead of print
7. Quäschling U, Kläver M, Richter C, Hamerla G, Mucha S, Scherlach C. Flow diversion in challenging vascular anatomies: The use of low profile stent retrievers for safe and accurate positioning of the microcatheter. CVIR Endovasc. 2020. 3: 19
8. Tokuyama K, Kiyosue H, Hori Y, Okahara M, Nagatomi H, Asayama Y. Utility of a steerable microcatheter for the selective transvenous embolization of dural arteriovenous fistulas. J Neuroendovasc Ther. 2023. 17: 153-8
9. Wang CC, Lv N, Feng ZZ, Li ZF, Zhao R, Li Q. Intraaneurysmal microcatheter looping technique for stent-assisted embolization of complex intracranial aneurysms. Interv Neuroradiol. 2015. 21: 580-4

