

- College of Medicine, Drexel University, Philadelphia, PA, USA
- Department of Neurosurgery, Allegheny Health Network Neuroscience Institute, Pittsburgh, PA, USA
- Center for Pain Relief, Allegheny Health Network, McMurray, PA, USA.
Correspondence Address:
Nisha L. Busch, College of Medicine, Drexel University, Philadelphia, PA, USA.
DOI:10.25259/SNI_696_2023
Copyright: © 2024 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Nisha L. Busch1, Nathan Esplin2, Michael Patterson3, Nestor D. Tomycz2. Successful relief of central poststroke pain with BurstDR spinal cord stimulation: A case series. 23-Feb-2024;15:60
How to cite this URL: Nisha L. Busch1, Nathan Esplin2, Michael Patterson3, Nestor D. Tomycz2. Successful relief of central poststroke pain with BurstDR spinal cord stimulation: A case series. 23-Feb-2024;15:60. Available from: https://surgicalneurologyint.com/surgicalint-articles/12760/
Date of Submission
18-Aug-2023
Date of Acceptance
18-Jan-2024
Date of Web Publication
23-Feb-2024
Abstract
Background: Central poststroke pain (CPSP) is a commonly undertreated condition that can negatively impact a patient’s quality of life. The efficacy of spinal cord stimulation (SCS) for the treatment of CPSP is not established due to limited studies.
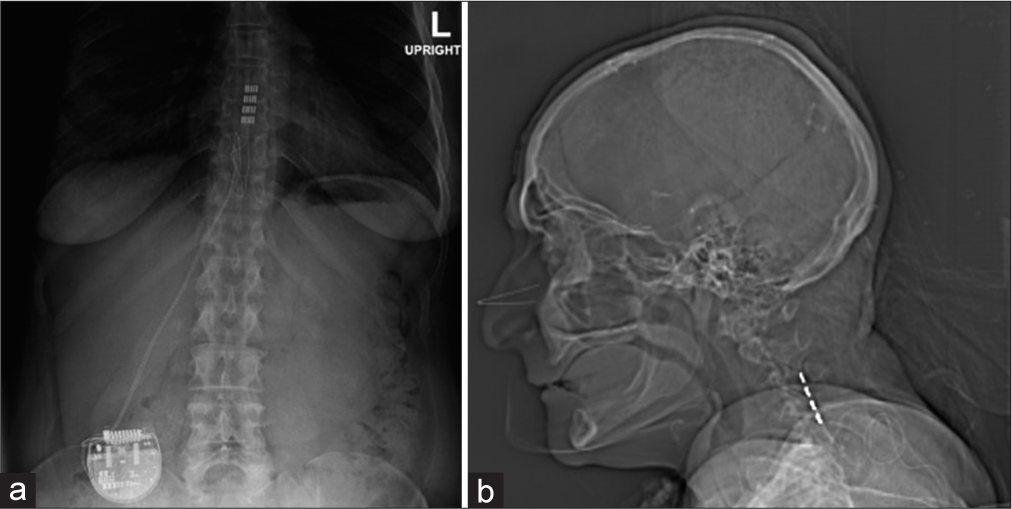
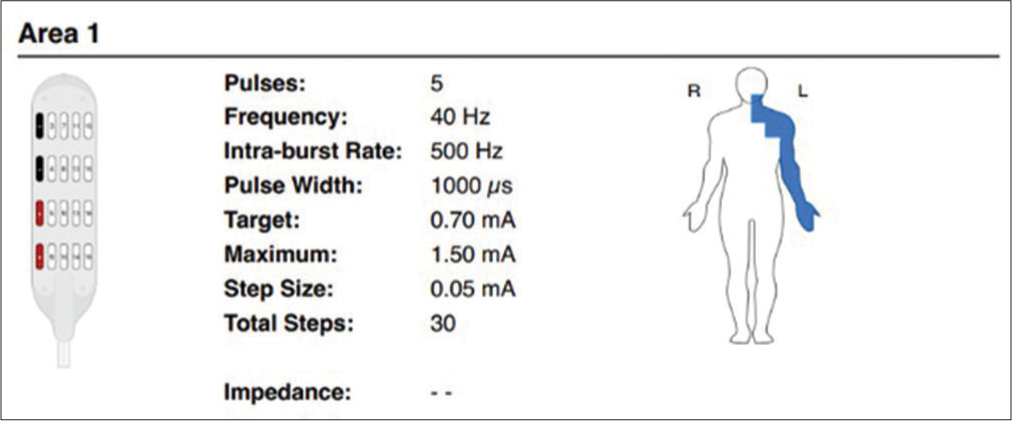
Case Description: Here, two patients, ages 42 and 75, sustained strokes resulting in CPSP. After failed medical management, both underwent placement of paddle-lead SCS systems utilizing BurstDR stimulation that successfully resulted in pain resolution.
Conclusion: Two patients with CPSP were successfully treated with paddle lead SCS with BurstDR programming.
Keywords: BurstDR, Central poststroke pain, Neuropathic pain, Spinal cord stimulation, Stroke
INTRODUCTION
Central poststroke pain (CPSP) is a commonly undertreated poststroke sequela that can significantly decrease a patient’s quality of life.[
CASE 1
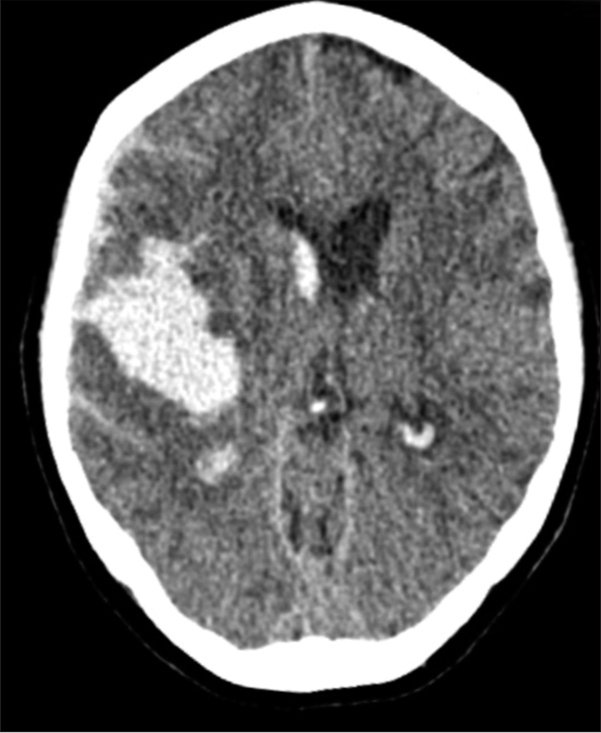
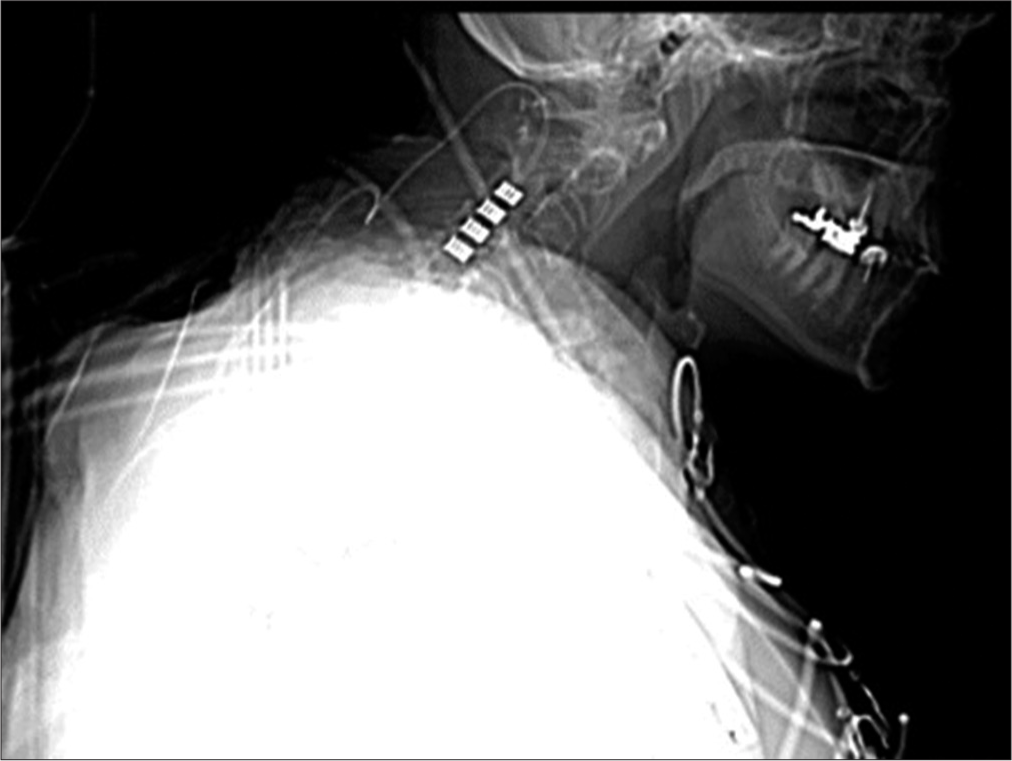
A 42-year-old female originally presented with a ruptured right middle cerebral artery (MCA) aneurysm treated with successful aneurysm clipping and subsequent cranioplasty [
CASE 2
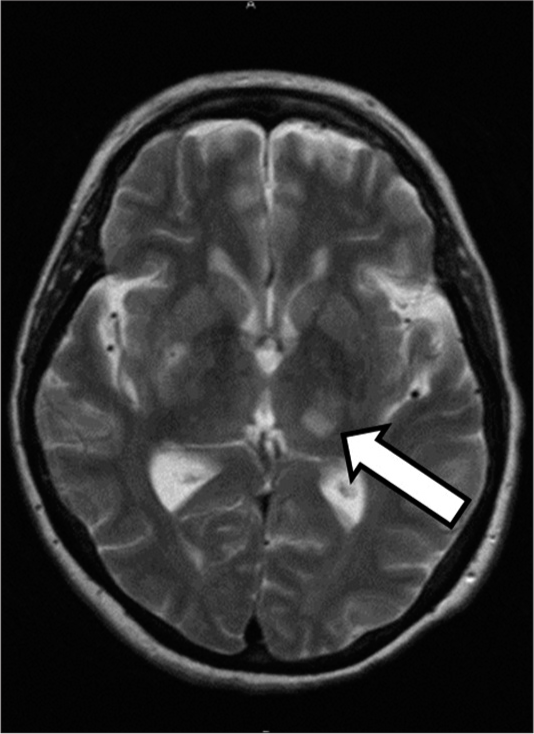
A 75-year-old female had an ischemic stroke involving the M1 segment of the right MCA. Following endovascular treatment, she was discharged to inpatient rehabilitation on aspirin and Plavix. One week later, she additionally sustained a left thalamic MCA stroke, resulting in weakness, an abnormal gait, aphasia, and a CPSP [
DISCUSSION
Mechanism of CPSP and treatment with SCS
CPSP occurs when a stroke results in a lesion of the spinothalamic tract (STT) of the central nervous system.[
CPSP treated with SCS
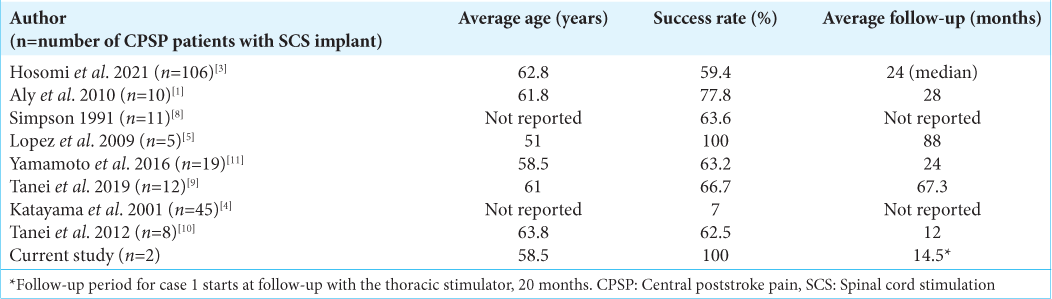
We identified eight case series of CPSP patients treated with SCS [
CONCLUSION
We present two cases of CPSP successfully treated with the implantation of paddle lead SCS with BurstDR programming.
Ethical approval
Institutional review board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
Dr. Nestor D. Tomycz: Dr. Nestor D. Tomycz serves as a consultant for and receives grant support from Abbott Neuromodulation. He serves on the surgeon advisory board for Boston Scientific. The remaining authors have no conflicts of interest to report.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Journal or its management. The information contained in this article should not be considered to be medical advice; patients should consult their own physicians for advice as to their specific medical needs.
References
1. Aly MM, Saitoh Y, Hosomi K, Oshino S, Kishima H, Yoshimine T. Spinal cord stimulation for central poststroke pain. Neurosurgery. 2010. 67: ons206-12 discussion ons212
2. Heijmans L, Joosten EA. Mechanisms and mode of action of spinal cord stimulation in chronic neuropathic pain. Postgrad Med. 2020. 132: 17-21
3. Hosomi K, Yamamoto T, Agari T, Takeshita S, Tanei T, Imoto H. Benefit of spinal cord stimulation for patients with central post-stroke pain: A retrospective multicenter study. J Neurosurg. 2022. 136: 601-12
4. Katayama Y, Yamamoto T, Kobayashi K, Kasai M, Oshima H, Fukaya C. Motor cortex stimulation for post-stroke pain: Comparison of spinal cord and thalamic stimulation. Stereotact Funct Neurosurg. 2001. 77: 183-6
5. Lopez JA, Torres LM, Gala F, Iglesias I. Spinal cord stimulation and thalamic pain: Long-term results of eight cases. Neuromodulation. 2009. 12: 240-3
6. Mohanan AT, Nithya S, Nomier Y, Hassan DA, Jali AM, Qadri M. Stroke-induced central pain: Overview of the mechanisms, management, and emerging targets of central post-stroke pain. Pharmaceuticals (Basel). 2023. 16: 1103
7. Payton H, Soundy A. The experience of post-stroke pain and the impact on quality of life: An integrative review. Behav Sci (Basel). 2020. 10: 128
8. Simpson BA. Spinal cord stimulation in 60 cases of intractable pain. J Neurol Neurosurg Psychiatry. 1991. 54: 196-9
9. Tanei T, Kajita Y, Takebayashi S, Aoki K, Nakahara N, Wakabayashi T. Predictive factors associated with pain relief of spinal cord stimulation for central post-stroke pain. Neurol Med Chir (Tokyo). 2019. 59: 213-21
10. Tanei T, Nakahara N, Takebayashi S, Hirano M, Kajita Y, Wakabayashi T. Dual lead spinal cord stimulation using octad lead for central post-stroke pain. No Shinkei Geka. 2012. 40: 325-9
11. Yamamoto T, Watanabe M, Obuchi T, Kano T, Kobayashi K, Oshima H. Importance of pharmacological evaluation in the treatment of poststroke pain by spinal cord stimulation. Neuromodulation. 2016. 19: 744-51

