

- Department of Neurosurgery, CHU Ibn Sina, Rabat, Morocco.
Correspondence Address:
Michèle Yolande Moune, Department of Neurosurgery, CHU Ibn Sina, Rabat, Morocco.
DOI:10.25259/SNI_1227_2021
Copyright: © 2022 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Michèle Yolande Moune1, Christine Milena Sayore1, Mustapha Hemama1, Nizare El Fatemi1, Moulay-Rachid El Maaqili1. Surgical management of a thoracic chordoma: A case report and literature review. 18-Feb-2022;13:63
How to cite this URL: Michèle Yolande Moune1, Christine Milena Sayore1, Mustapha Hemama1, Nizare El Fatemi1, Moulay-Rachid El Maaqili1. Surgical management of a thoracic chordoma: A case report and literature review. 18-Feb-2022;13:63. Available from: https://surgicalneurologyint.com/surgicalint-articles/11395/
Date of Submission
11-Dec-2021
Date of Acceptance
19-Jan-2022
Date of Web Publication
18-Feb-2022
Abstract
Background: Chordomas are rare benign, but locally aggressive tumors that are regularly encountered in the clivus and sacrum. Although they are rarely found in the thoracic spine, they can contribute not only to local bone destruction and spinal instability, lead to cord compression, and major neurological deficits.
Case Description: A 56 year-old-male originally underwent a T12 laminectomy with debulking for a thoracic chordoma. Two years later, the lesion recurred contributing to a significant paraparesis. The new MR showed a T2 hyper intense lesion with huge epidural extension that warranted a 360° surgical decompression and fusion. The histopathology from both surgeries confirmed the diagnosis of a chordoma.
Conclusion: Combined 360° decompression and fusion was warranted to resect a T12 chordoma that recurred 2 years following an original laminectomy with debulking procedure.
Keywords: Combined anterior and posterior approach, Recurrence, Spinal surgery, Thoracic chordoma
INTRODUCTION
Chordomas are slow-growing but locally invasive/aggressive lesions that account for 2–4% of all primary malignant bone tumors.[
CASE STUDY
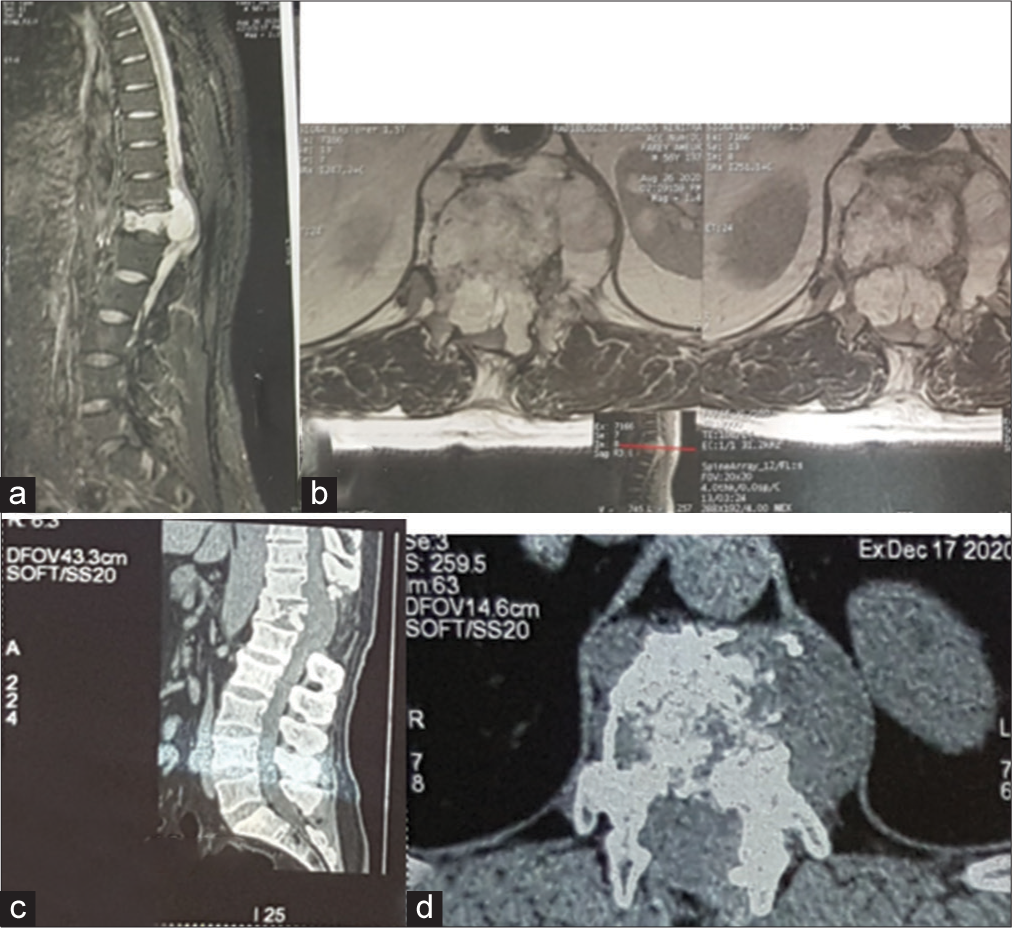
A 56-year-old male presented 2 years ago with T12-dorsal/intercostal pain. The MR documented an enhancing T12 vertebral lesion with ventral epidural extension contributing to marked cord compression [

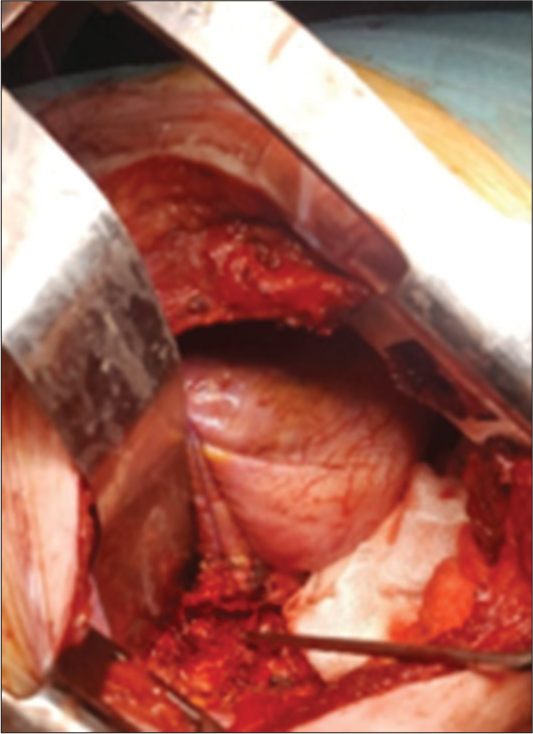
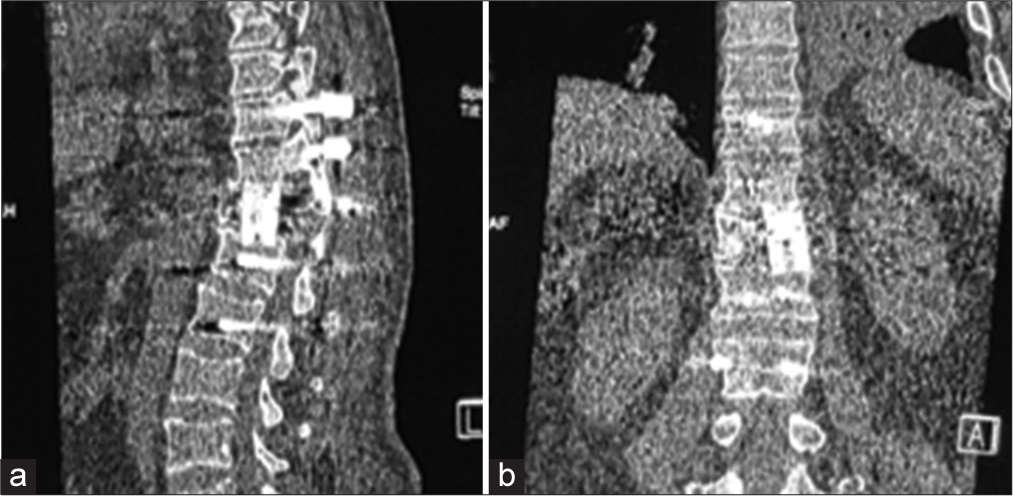
Recurrence of T12 chordoma 2 years later requiring 360° decompression/fusion
Two years later, the patient presented with recurrent dorsal pain, and a significant para paresis (i.e., motor exam 3–4/5 right leg/4–5/5 left leg, diffuse hyperreflexia, and T12 pin level, and anal incontinence). Thoracic and lumbar MRI/CT studies documented a lytic T12 vertebral body lesion with a large ventral canal extradural mass contributing to severe cord compression [
DISCUSSION
Chordomas represent 2–4% of primary malignant bone tumors.[
Adjunctive radiation therapy (RT) and chemotherapy for chordomas
Chordomas are relatively radioresistant; although RT increases disease-free survival it does not prevent recurrence.[
Recurrence rate for chordomas
Chordomas recur in up to 25–89% of cases (i.e., dependent on their original location).[

CONCLUSION
Despite gross total, en bloc resection, spinal chordomas still recur in up to 66% of cases. Here, 2 years following an original decompression/partial debulking of a T12 lesion, the patient underwent a definitive 360° en bloc resection (decompression/ fusion) followed by appropriate adjunctive treatment.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
The author thanks Dr. Djoubairou Ben for writing assistance.
References
1. Ahmed R, Sheybani A, Menezes AH, Buatti JM, Hitchon PW. Disease outcomes for skull base and spinal chordomas: A single center experience. Clin Neurol Neurosurg. 2015. 130: 67-73
2. Bakker SH, Jacobs WC, Pondaag W, Gelderblom H, Nout RA, Dijkstra PD. Chordoma: A systematic review of the epidemiology and clinical prognostic factors predicting progression-free and overall survival. Eur Spine J. 2018. 27: 3043-58
3. Boriani S, Bandiera S, Biagini R, Bacchini P, Boriani L, Cappuccio M. Chordoma of the mobile spine: Fifty years of experience. Spine. 2006. 31: 493-503
4. D’Amore T, Boyce B, Mesfin A. Chordoma of the mobile spine and sacrum: Clinical management and prognosis. J Spine Surg. 2018. 4: 546-52
5. Denaro L, Berton A, Ciuffreda M, Loppini M, Candela V, Brandi ML. Surgical management of chordoma: A systematic review. J Spinal Cord Med. 2020. 43: 797-812
6. Liu S, Zhou X, Song A, Huo Z, Yao S, Wang Y. Surgical treatment of giant chordoma in the thoracic spine combining thoracoscopic and posterior spinal surgery: A case report. Medicine (Baltimore). 2019. 98: e16990
7. Oppenlander ME, Maulucci CM, Ghobrial GM, Evans NR, Harrop JS, Prasad SK. En bloc resection of upper thoracic chordoma via a combined simultaneous anterolateral thoracoscopic and posterior approach. Oper Neurosurg. 2014. 10: 380-6
8. Pu F, Wang B, Liu J, Chen F, Shao Z. Giant chordoma in the thoracolumbar spine: A case report and literature review. Eur Spine J. 2017. 26: 95-9
9. Sciubba DM, Chi JH, Rhines LD, Gokaslan ZL. Chordoma of the spinal column. Neurosurg Clin N Am. 2008. 19: 5-15

