

- Pars Advanced and Minimally Invasive Medical Manners Research Center, Pars Hospital, Iran University of Medical Sciences, Tehran, Iran.
DOI:10.25259/SNI_592_2019
Copyright: © 2020 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Abolfazl Rahimizadeh, Valiollah Hassani, Housain Soufiani, Ava Rahimizadeh, Mona Karimi, Naser Asgari. Symptomatic pulmonary cement embolism after pedicle screw polymethylmethacrylate cement augmentation: A case report and review. 07-Feb-2020;11:18
How to cite this URL: Abolfazl Rahimizadeh, Valiollah Hassani, Housain Soufiani, Ava Rahimizadeh, Mona Karimi, Naser Asgari. Symptomatic pulmonary cement embolism after pedicle screw polymethylmethacrylate cement augmentation: A case report and review. 07-Feb-2020;11:18. Available from: https://surgicalneurologyint.com/surgicalint-articles/9865/
Date of Submission
10-Dec-2019
Date of Acceptance
08-Jan-2020
Date of Web Publication
07-Feb-2020
Abstract
Background: In osteoporotic patients, a useful technique for significantly enhancing the strength of a pedicle screw is augmentation with polymethylmethacrylate cement. However, a rare complication of this procedure is a symptomatic pulmonary cement embolism.
Case Description: A pedicle screw cement augmentation was performed in a middle-aged female for the failed back syndrome. When she developed symptomatic pulmonary cement emboli, she was successfully managed with conservative measures, including anticoagulation.
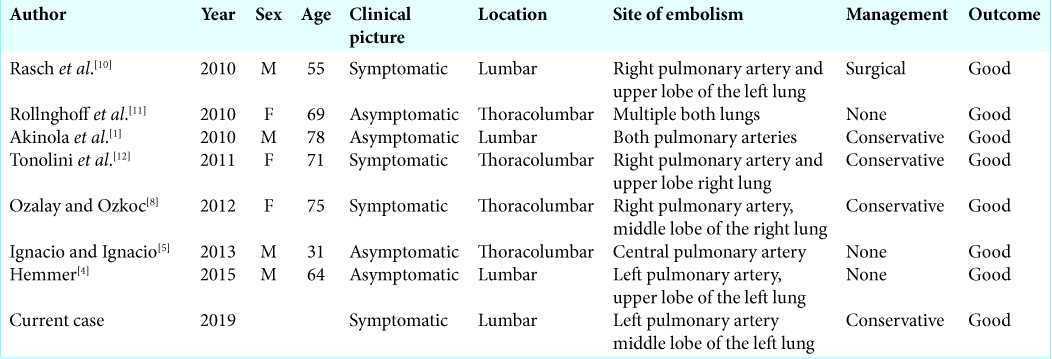
Conclusion: Despite the increased use of cement augmentation for pedicle screw placement and the relatively high incidence of cement leakage into the prevertebral venous system, symptomatic cement pulmonary embolism remains rare. The management of such symptomatic CPE should be evaluated and treated based on both the size and location of the embolism. Here, we presented this case while reviewing three symptomatic and four asymptomatic cases from the literature.
Keywords: Cement augmentation, Cement pulmonary emboli, Complication, Failed back syndrome, Pedicle screw, Polymethylmethacrylate
INTRODUCTION
For nearly two decades, polymethylmethacrylate (PMMA) augmentation of pedicle screws in osteoporotic patients has been performed to improve pullout strength. One of the very rare but serious complications is symptomatic pulmonary cement embolism (PCE).[
CASE REPORT
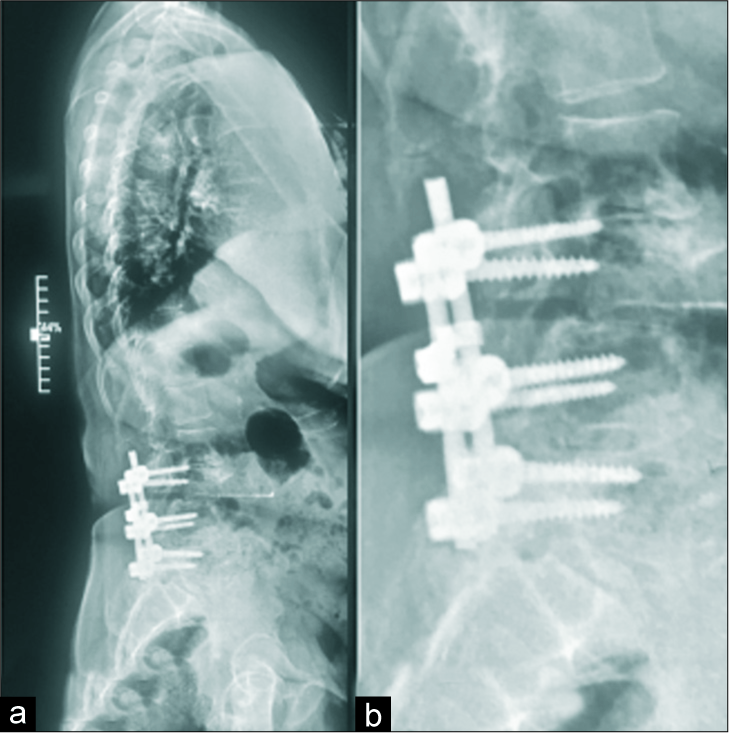
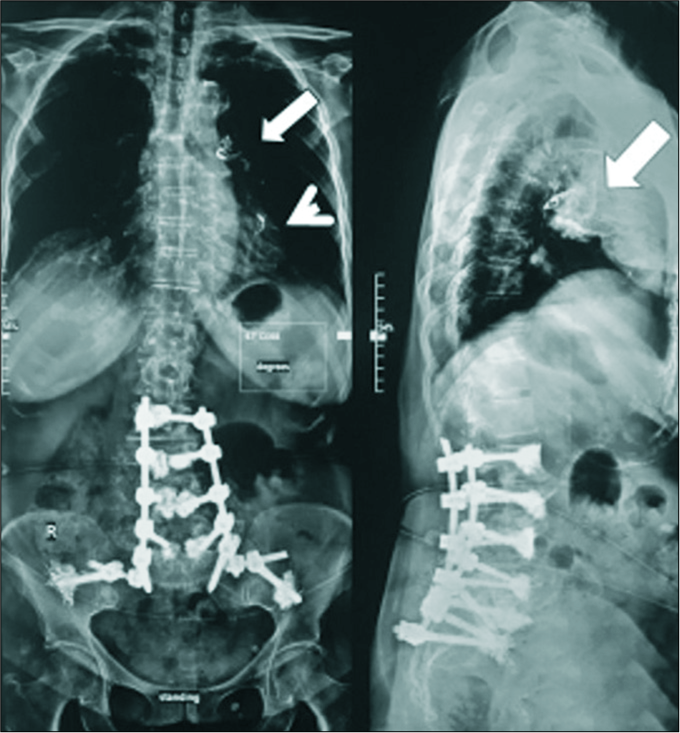
A middle-aged female underwent surgery for failed back syndrome requiring additional decompression and instrumentation [
DISCUSSION
One of the most serious complications of pedicle screw PMMA augmentation is cement leakage into the inferior vena cava or azygos vein with subsequent migration through the pulmonary arteries into the lungs (e.g., PCE).[
Risk factors and prevention
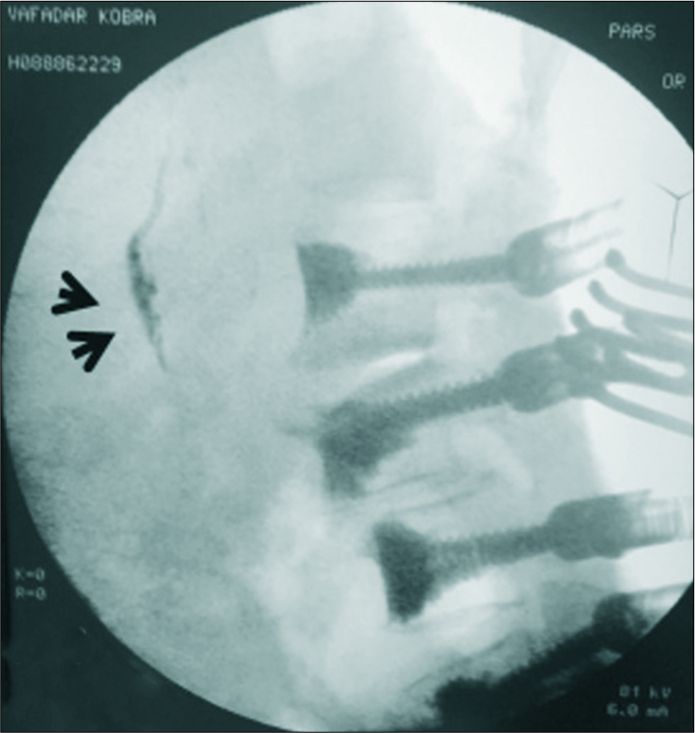
The occurrence of PCE during pedicle screw PMMA augmentation depends on the viscosity of cement at the time of its delivery. The increased force attributed to the rapid injection of low viscous cement (dough-like) likely contributes to a higher incidence of PCE, while the reduced delivery rate of toothpaste-like cement results in a smaller incidence of leakage.[
Clinical picture of PCE
The clinical picture of a symptomatic PCE is similar to that of a thrombotic PE; the cardinal features include tachycardia, dyspnea, hypotension, and loss of consciousness that may result in cardiorespiratory arrest and death.[
Diagnostic imaging
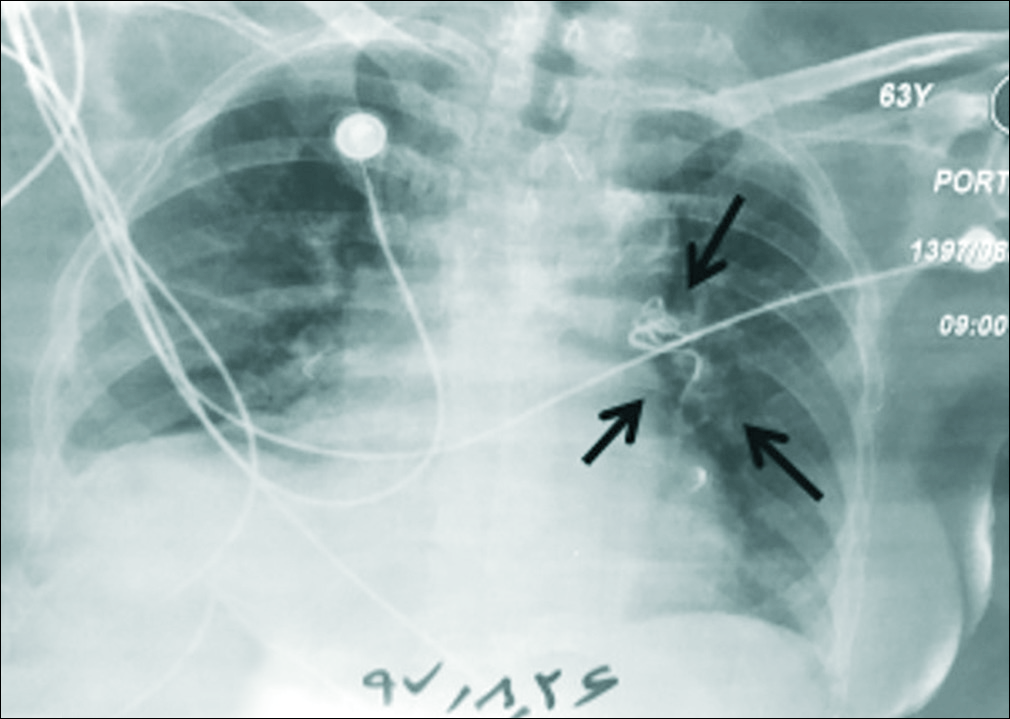
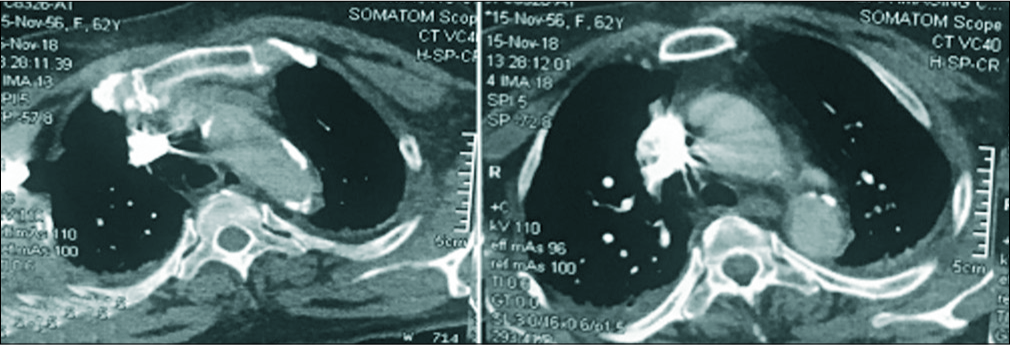
With PCE, echocardiography may demonstrate changes in pulmonary artery pressure and right ventricular dilatation. The chest X-ray and CT for both symptomatic and asymptomatic PCE may be visualized as large tubular, branching (serpentine), or multiple small densities/opacities.[
Management
Asymptomatic subjects with small cement particles in the lung fields require no treatment, while those with symptomatic thrombotic pulmonary emboli require emergent anticoagulation, for example, 5000 units of heparin and IV push followed by 1000 units/h.[
CONCLUSION
Symptomatic PCE is a rare, potentially catastrophic complication of augmenting pedicle screw instrumentation with PMMA. Rapidly injected low-viscous cement significantly contributes to cement leakage. If studies (X-ray, chest CT, and CT angiography) demonstrate cement in the inferior vena cava, one should be aware of its potential for embolization into the lungs (e.g., PCE).
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Akinola B, Lutchman L, Barker P, Rai A. Pulmonary cement embolism during cement augmentation of pedicle screw fixation: A case report. J Orthop Surg (Hong Kong). 2010. 18: 364-6
2. Baroud G, Crookshank M, Bohner M. High-viscosity cement significantly enhances uniformity of cement filling in vertebroplasty: An experimental model and study on cement leakage. Spine (Phila Pa 1976). 2006. 31: 2562-8
3. El Saman A, Kelm A, Meier S, Sander AL, Eichler K, Marzi I. Intraoperative PEEP-ventilation during PMMA-injection for augmented pedicle screws: Improvement of leakage rate in spinal surgery. Eur J Trauma Emerg Surg. 2013. 39: 461-8
4. Hemmer C. Abnormal chest X-ray and computed tomography post-lumbar fusion. J Nurse Pract. 2015. 11: 276-8
5. Ignacio J, Ignacio SD. Pulmonary bone cement embolism following pedicle screw instrumentation with bone cement augmentation for a burst fracture of l1 in a non-osteoporotic spine. Acta Med Philipp. 2013. 47: 76-79
6. Janssen I, Ryang YM, Gempt J, Bette S, Gerhardt J, Kirschke JS. Risk of cement leakage and pulmonary embolism by bone cement-augmented pedicle screw fixation of the thoracolumbar spine. Spine J. 2017. 17: 837-44
7. Kim YJ, Lee JW, Park KW, Yeom JS, Jeong HS, Park JM. Pulmonary cement embolism after percutaneous vertebroplasty in osteoporotic vertebral compression fractures: Incidence, characteristics, and risk factors. Radiology. 2009. 251: 250-9
8. Ozalay MO. Pulmonary cement embolism after segmental polymethyl methacrylate augmented pedicle screw fixation. J Turk Spinal Surg. 2012. 23: 233-240
9. Rahimizadeh A, Malekmohammadi Z, Williamson WL, Rahimizadeh S, Amirzadeh M, Asgari N. Rivaroxaban-induced acute cervical spine epidural hematoma: Report of a case and review. Surg Neurol Int. 2019. 10: 210-
10. Rasch A, Sindermann J, Scheld HH, Hoffmeier A. Pulmonary palacos embolism: A case report. Thorac Cardiovasc Surg. 2010. 58: 437-9
11. Röllinghoff M, Siewe J, Eysel P, Delank KS. Pulmonary cement embolism after augmentation of pedicle screws with bone cement. Acta Orthop Belg. 2010. 76: 269-73
12. Tonolini M, Bianco R. Pulmonary cement embolism after pedicle screw vertebral stabilization. J Emerg Trauma Shock. 2012. 5: 272-3
13. Ulusoy OL, Kahraman S, Karalok I, Kaya E, Enercan M, Sever C. Pulmonary cement embolism following cement-augmented fenestrated pedicle screw fixation in adult spinal deformity patients with severe osteoporosis (analysis of 2978 fenestrated screws). Eur Spine J. 2018. 27: 2348-56

