

- Department of Neurosurgery, Fukuoka Neurosurgical Hospital, Fukuoka, Japan.
- Department of Cerebrovascular Medicine, Fukuoka Neurosurgical Hospital, Fukuoka, Japan.
Correspondence Address:
Kaisei Kamatani, Department of Neurosurgery, Fukuoka Neurosurgical Hospital, Fukuoka, Japan.
DOI:10.25259/SNI_525_2023
Copyright: © 2023 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Kaisei Kamatani1, Shinichiro Yoshida1, Noriaki Tashiro2, Yoshiya Hashiguchi2, Kousuke Takigawa1, Masahiro Yasaka2, Hiroshi Aikawa1, Yoshinori Go1, Kiyoshi Kazekawa1. The case of treatment for carotid web – Double-layer micromesh stent implantation in our hospital. 15-Sep-2023;14:339
How to cite this URL: Kaisei Kamatani1, Shinichiro Yoshida1, Noriaki Tashiro2, Yoshiya Hashiguchi2, Kousuke Takigawa1, Masahiro Yasaka2, Hiroshi Aikawa1, Yoshinori Go1, Kiyoshi Kazekawa1. The case of treatment for carotid web – Double-layer micromesh stent implantation in our hospital. 15-Sep-2023;14:339. Available from: https://surgicalneurologyint.com/surgicalint-articles/12548/
Date of Submission
20-Jun-2023
Date of Acceptance
26-Aug-2023
Date of Web Publication
15-Sep-2023
Abstract
Background: A carotid web is a shelf-like structure on the posterior wall of the origin of the internal carotid artery, and it is believed to cause cerebral infarction due to thrombus formed by turbulent flow with stagnation of blood flow. Recently, it has been suggested that recurrent cerebral infarction cannot be prevented in patients with a symptomatic carotid web by conventional medical management alone. However, there is still no consensus on the treatment of carotid webs. Carotid artery stenting (CAS) with the CASPER stent (Microvention, Terumo, Tustin, CA, USA) was performed in six consecutive patients with symptomatic carotid webs, and the results are reported along with a review of the literature.
Methods: Six consecutive patients with a diagnosis of internal carotid artery stenosis due to a carotid web on magnetic resonance imaging and digital subtraction angiography (DSA) were included in this study. All patients underwent dual antiplatelet therapy approximately 10 days before surgery and after 6 months, and then, a CASPER stent was implanted under general anesthesia. All patients were evaluated postoperatively by DSA 6 months after treatment.
Results: In all patients, no in-stent stenosis was seen 6 months after the operation, and no symptomatic cerebral infarction occurred within 1 year after the procedure.
Conclusions: CASPER stent implantation may be effective for treating carotid webs.
Keywords: Carotid web, Stent, Stroke
INTRODUCTION
A carotid web is a shelf-like structure on the posterior wall of the origin of the internal carotid artery, and it is believed to cause cerebral infarction due to a thrombus formed by turbulent flow with stagnation of blood flow.[
The CASPER stent is a self-expandable nitinol stent with a dual-layer structure of tubular mesh. The outer layer consists of a braided closed-cell structure with close vessel wall apposition and good conformability, and the inner layer has a closed-cell design with a very small micromesh to limit plaque prolapse and embolic release. The dual-layer structure was considered to be effective against fibrotic and ulcerative lesions. Carotid artery stenting (CAS) was performed using the CASPER stent (Microvention, Terumo, Tustin, CA, USA) in six consecutive patients with symptomatic carotid webs. The results of the treatment at our hospital are reported along with a review of the literature.
METHODS
Of the patients diagnosed with cerebral infarction at our hospital between October 2020 and May 2022, six consecutive patients diagnosed with carotid artery stenosis on magnetic resonance imaging (MRI) and digital subtraction angiography (DSA) were included. The diagnosis of a carotid web in the lesion was made based on the previous literature[
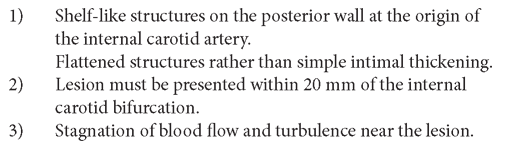
Figure 1:
Images of a representative case. (a) MRI: Cerebral infarction of the right frontal lobe is observed; (b) MRA: A low-intensity linear structure protruding anteriorly from the posterior wall of the origin of the right internal carotid artery is observed (arrow). (c) T1 black-blood scan. Linear structures are visualized as slightly high-intensity lesions (arrow). (d) DSA. A linear shadow defect extending anteriorly from the posterior wall of the origin of the right internal carotid artery is observed (arrow).
CASE PRESENTATION
The patient is an 80-year-old male. On the day of admission, he suddenly noticed dysphasia and weakness in the left upper and lower limbs and was transported to our hospital. Head MRI showed a new cerebral infarction at the right frontal lobe and wall irregularity of the right internal carotid artery. DSA showed a shelf-like lesion at the origin of the right internal carotid artery, so we diagnosed it as a carotid web. Echocardiography showed no abnormal findings that could be the source of the embolus, and a computed tomography scan of the thorax and abdomen denied malignant disease, so the cerebral infarction was thought to be caused by a carotid web. CAS was performed on the 17th day.
RESULTS
The mean age of this case group was 81.3 years. Five cases had hypertension and fur cases had hyperlipidemia [
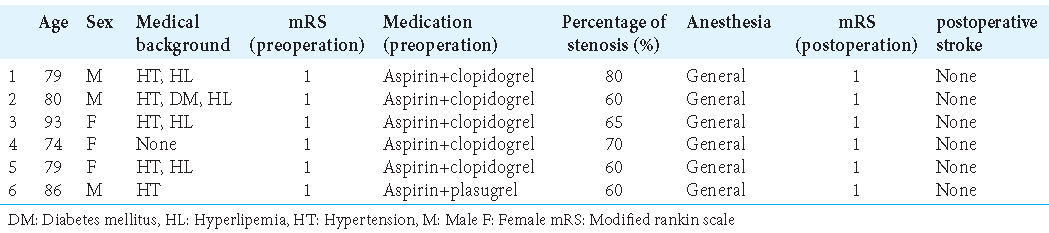
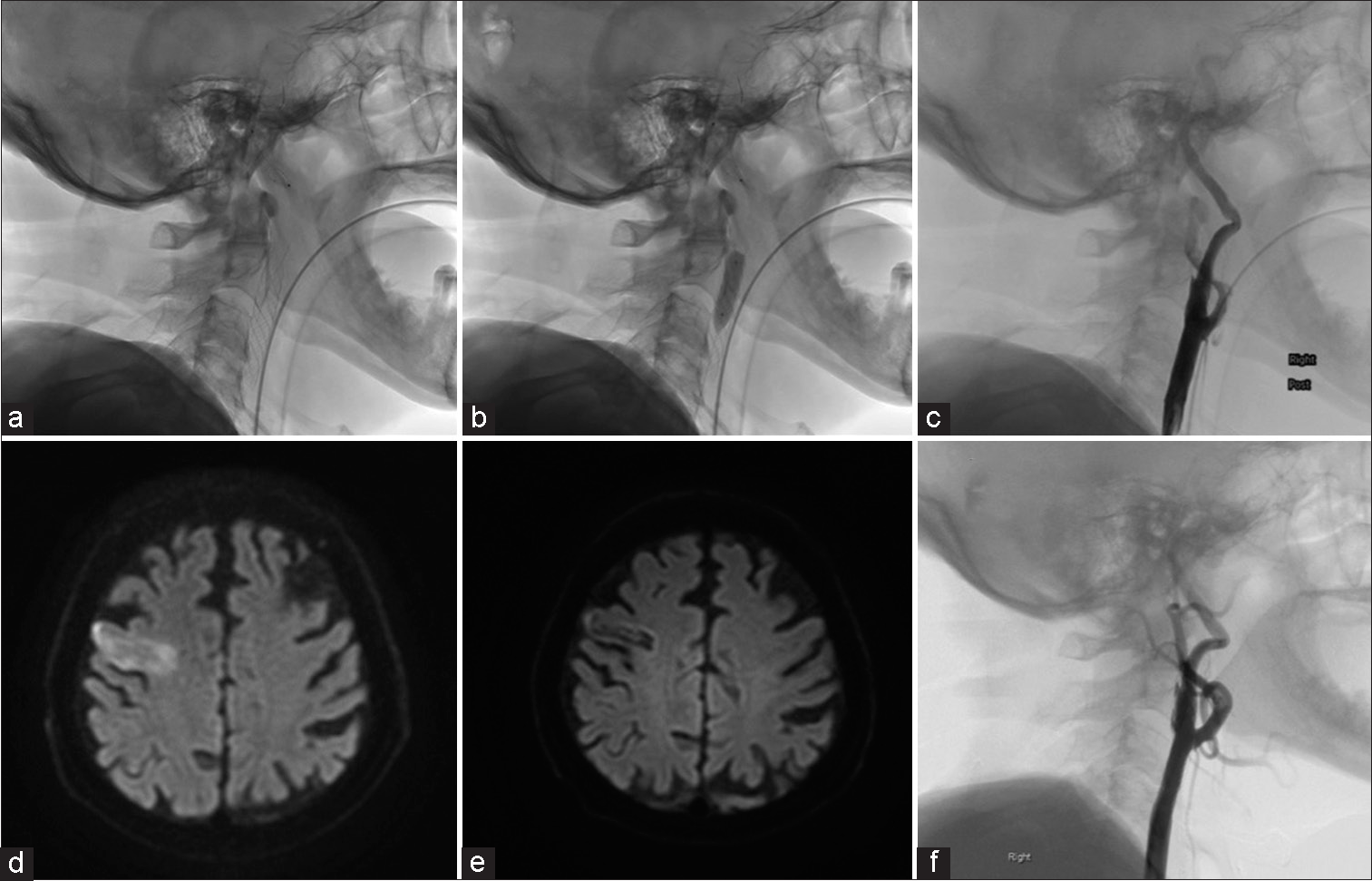
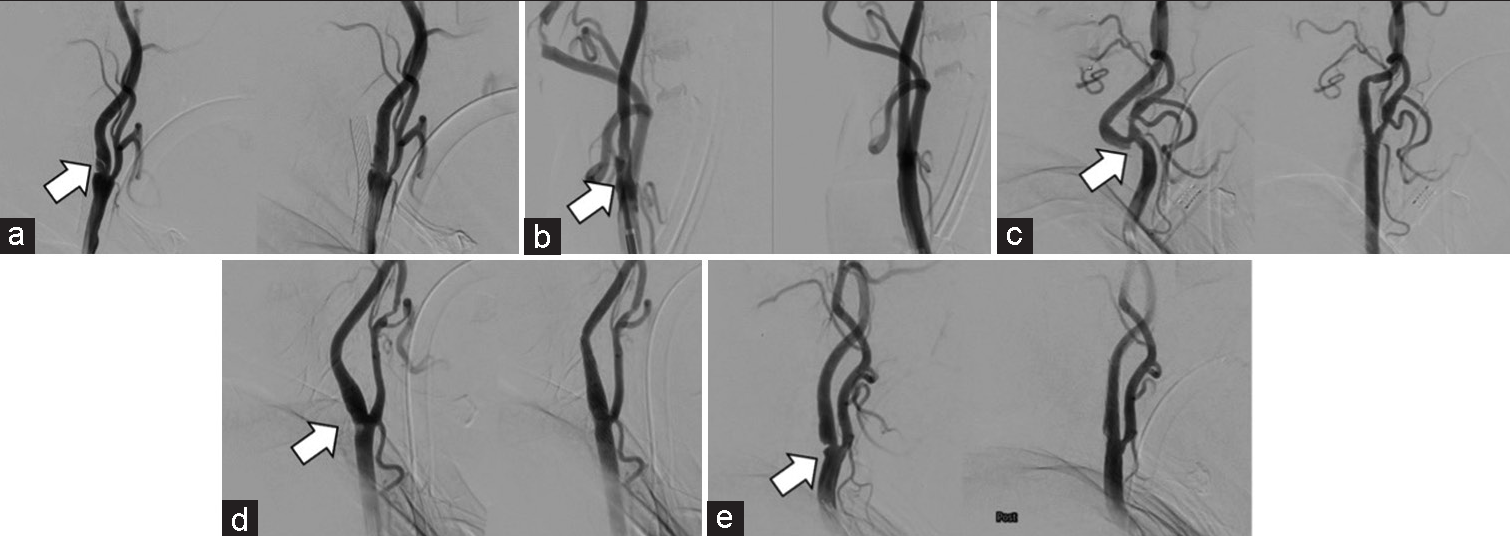
Figure 2:
Intraoperative findings of CAS. (a) Full deployment of a CASPER stent. (b) Post dilation. (c) Postoperative DSA. No acute instent occlusion or plaque protrusion is observed. (d) Postoperative MRI. No ischemic complications are observed. (e) MRI 6 months after treatment. No new infarction is observed. (f) DSA 6 months after treatment. No in-stent stenosis is observed.
DISCUSSION
A carotid web is defined as a shelf-like structure on the posterior wall of the origin of the internal carotid artery, and it has been reported to show fibromuscular dysplasia of the vascular intima, unrelated to atherosclerotic factors. It is not known why carotid webs occur at these sites.[
A carotid web protrudes into the internal carotid artery, and its membranous structure causes turbulent flow with stagnant blood flow at the isthmus of the lesion, which increases the risk of platelet aggregation, and thrombus formed there is said to cause cerebral infarction.[
The presence of stagnant blood flow near the lesion is also a criterion for the diagnosis of a carotid web in our hospital [
Patients with cerebral infarction who have a carotid web are considered to be at high risk for recurrent infarction. In a study by Guglielmi et al., one in six patients with a symptomatic carotid web had recurrent cerebral infarction within 2 years, suggesting that conventional medical treatment alone may not be sufficient to prevent recurrence.[
In a systematic review by Zhang et al., 54% of patients treated with antiplatelet therapy and 75% of patients treated with anticoagulation had a recurrence, whereas patients treated with surgical revascularization had no recurrence.[
The CASPER stent was performed in this study. Kawahara et al.[
To improve treatment safety, general anesthesia was performed in all CAS cases in this study. Nagata et al. have shown that general anesthesia using sevoflurane and nitrous oxide in oxygen-depressed baroreceptor reflex sensitivity, induced hemodynamic stability under CAS, and may decrease the rate of occurrence of complications.[
CONCLUSION
Although this was a single-center study with a small number of cases, it showed that CAS with a CASPER stent for symptomatic carotid webs did not cause ischemic complications. Thus, CAS with a CASPER stent may be an effective treatment for a symptomatic carotid web. We hope that this paper will be useful for future studies of the treatment of symptomatic carotid webs.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The author(s) confirms that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Journal or its management. The information contained in this article should not be considered to be medical advice; patients should consult their own physicians for advice as to their specific medical needs.
References
1. Gekka M, Osanai T, Aoki T, Nakayama N, Kazumata K, Houkin K. Efficacy of carotid artery stenting performed under general anesthesia with somatosensory evoked potential monitoring. J Stroke Cerebrovasc Dis. 2021. 30: 106007
2. Guglielmi V, Compagne KC, Sarrami AH, Sluis WM, van den Berg LA, van der Sluijs PM. Assessment of recurrent stroke risk in patients with a carotid web. JAMA Neurol. 2021. 78: 826-33
3. Haussen DC, Grossberg JA, Koch S, Malik A, Yavagal D, Gory B. Multicenter experience with stenting for symptomatic carotid web. Interv Neurol. 2018. 7: 413-8
4. Imamura H, Sakai N, Matsumoto Y, Yamagami H, Terada T, Fujinaka T. Clinical trial of carotid artery stenting using dual-layer CASPER stent for carotid endarterectomy in patients at high and normal risk in the Japanese population. J Neurointerv Surg. 2021. 13: 524-9
5. Janzen J. The microscopic transitional zone between elastic and muscular arteries. Arch Mal Coeur Vaiss. 2004. 97: 909-14
6. Kawahara I, Hiu T, Ono T, Haraguchi W, Ushijima R, Tsutsumi K. Reconsideration of carotid web and the therapeutic strategy. No Shinkei Geka. 2019. 47: 659-66
7. Krasteva MP, Diamantaras AA, Siller T, Mordasini P, Heldner MR. Symptomatic carotid web in a female patient. SAGE Open Med Case Rep. 2020. 8:
8. Lenck S, Labeyrie MA, Mosimann PJ, Saint-Maurice JP, Houdart E. Diaphragm of the internal carotid artery: A novel cause of pulsatile tinnitus. J Neurol. 2013. 260: 2185-7
9. Mac Grory B, Emmer BJ, Roosendaal SD, Zagzag D, Yaghi S, Nossek E. Carotid web: An occult mechanism of embolic stroke. J Neurol Neurosurg Psychiatry. 2020. 91: 1283-9
10. Nagata S, Kazekawa K, Aikawa H, Tsutsumi M, Kodama T, Iko M. Hemodynamic stability under general anesthesia in carotid artery stenting. Radiat Med. 2005. 23: 427-31
11. Yamada K, Yoshimura S, Miura M, Kanamaru T, Shindo S, Uchida K. Potential of new-generation double-layer micromesh stent for carotid artery stenting in patients with unstable plaque: A preliminary result using OFDI analysis. World Neurosurg. 2017. 105: 321-6
12. Yang T, Yoshida K, Maki T, Fushimi Y, Yamada K, Okawa M. Prevalence and site of predilection of carotid webs focusing on symptomatic and asymptomatic Japanese patients. J Neurosurg. 2021. 135: 1370-6
13. Zhang AJ, Dhruv P, Choi P, Bakker C, Koffel J, Anderson D. A systematic literature review of patients with carotid web and acute ischemic stroke. Stroke. 2018. 49: 2872-6

