

- Department of Neurosurgery, Kindai University Faculty of Medicine, Osaka, Japan
- Department of Neurosurgery, Stroke Center, Teishinkai Hospital, Hokkaido, Japan
Correspondence Address:
Hisashi Kubota
Department of Neurosurgery, Kindai University Faculty of Medicine, Osaka, Japan
DOI:10.4103/2152-7806.183542
Copyright: © 2016 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Kubota H, Sanada Y, Tanikawa R, Kato A. The use of fibrin and gelatin fixation to repair a kinked internal carotid artery in carotid endarterectomy. Surg Neurol Int 03-Jun-2016;7:
How to cite this URL: Kubota H, Sanada Y, Tanikawa R, Kato A. The use of fibrin and gelatin fixation to repair a kinked internal carotid artery in carotid endarterectomy. Surg Neurol Int 03-Jun-2016;7:. Available from: http://surgicalneurologyint.com/surgicalint_articles/the-use-of-fibrin-and-gelatin-fixation-to-repair-a-kinked-internal-carotid-artery-in-carotid-endarterectomy/
Abstract
Background:The kinking of the internal carotid artery (ICA) after final closure in carotid endarterectomy (CEA) is thought to be uncommon. When it occurs, it is mandatory to reconstruct ICA to preserve normal blood flow. We herein present a case in which a fixation technique was applied to repair an ICA that became kinked during CEA.
Case Description:A 68-year-old man presented with cerebral infarction due to an artery-to-artery embolism from the right cervical ICA stenosis. CEA was performed 12 days after admission. After final closure, a distal portion of ICA was found to have been kinked following plaque resection in CEA procedure. Fixation with fibrin glue and gelatin was used to reinforce the arterial wall and repair the kink. Postoperative magnetic resonance angiography demonstrated the release of the kink in ICA.
Conclusion:Fixation with fibrin and gelatin is a salvage armamentarium that can be considered in CEA for the repair of kinked or tortuous ICA.
Keywords: Carotid endarterectomy, fibrin/gelatin fixation, internal carotid artery, kinking
INTRODUCTION
The course of the internal carotid artery (ICA) after carotid bifurcation shows many variations such as curves, kinks, and coils.[
CASE REPORT
A 68-year-old male with left hemiparesis admitted to our institute. Magnetic resonance imaging showed multiple spotty cerebral infarctions in the right middle cerebral artery. The right cervical ICA showed 75% stenosis with a plaque hemorrhage, which might have caused an artery-to-artery embolism. The cervical ICA showed a strong curved course in the medial direction after the stenotic lesion on magnetic resonance angiography (MRA) [
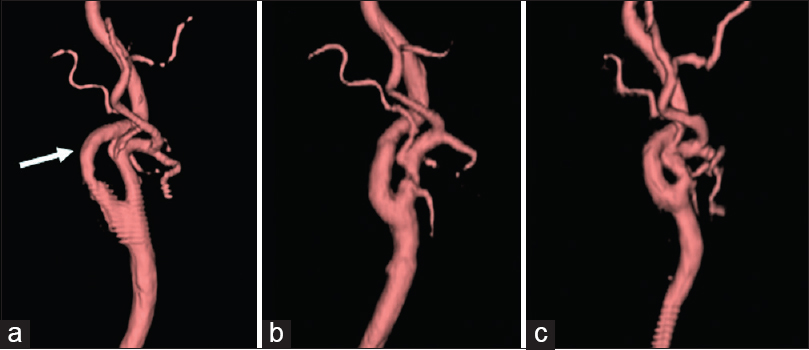
Figure 1
The right lateral view of the internal carotid artery depicted by magnetic resonance angiography volume rendering images. (a) Preoperative magnetic resonance angiography shows the internal carotid artery curved steeply in a medial direction after the stenosis (arrow). (b) Postoperative magnetic resonance angiography shows that the kinked internal carotid artery is properly reconstructed. (c) Magnetic resonance angiography at 1 year after the operation demonstrates that there is no restenosis and that the internal carotid artery shape was preserved
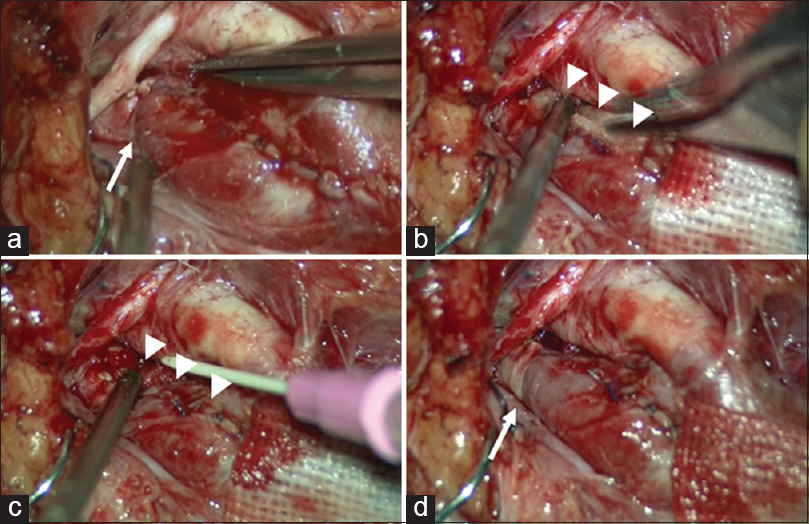
Figure 2
The intraoperative findings. (a) The internal carotid artery is kinked after plaque resection (arrow). (b) Fibrinogen-soaked gelatin (arrowheads) is used to reinforce the kinked internal carotid artery. (c) The fixation (arrowheads) in a medial wall of the internal carotid artery is completed with thrombin. (d) The kink is released (arrow)
DISCUSSION
The kinking of arteries after surgical manipulation can lead to a critical ischemic event. Yuan et al.[
However, allergic side effects have been reported.[
CONCLUSION
The utilization of fibrin and gelatin for the reconstruction of a kinked or tortuous ICA should be considered in CEA as a simple salvage method to reinforce the ICA wall and maintain cerebral blood flow.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Cheng YS, Lin PY, Lin KH, Ko CJ, Lin CC, Chen YL. Innovative technique for preventing hepatic artery kinking in living donor liver transplantation. Liver Transpl. 2013. 19: 664-5
2. Fundaró P, Velardi AR, Santoli C. Fibrin adhesive: Clinical application in coronary artery bypass graft surgery. Tex Heart Inst J. 1985. 12: 275-8
3. Imamaki M, Sakurai M, Shimura H, Ishida A, Fujita H, Miyazaki M. Pitfalls of skeletonized internal thoracic artery: Comparison of graft kinking between skeletonized and pedicled grafts based on postoperative angiography findings. J Card Surg. 2007. 22: 195-8
4. Kanazawa R, Sato S, Iwamoto N, Teramoto A. Allergic reaction following arachnoid plasty with a fibrin sealant. Neurol Med Chir (Tokyo). 2010. 50: 608-10
5. Kubota H, Tanikawa R, Katsuno M, Noda K, Ota N, Miyata S. Reconstruction of intracranial vertebral artery with radial artery and occipital artery grafts for fusiform intracranial vertebral aneurysm not amenable to endovascular treatment: Technical note. Acta Neurochir (Wien). 2013. 155: 1517-24
6. Paulsen F, Tillmann B, Christofides C, Richter W, Koebke J. Curving and looping of the internal carotid artery in relation to the pharynx: Frequency, embryology and clinical implications. J Anat. 2000. 197: 373-81
7. Purello-D’Ambrosio F, Gangemi S, La Rosa G, Merendino RA, Tomasello F. Allergy to gelatin. Allergy. 2000. 55: 414-5
8. Schwabegger AH, Engelhardt TO, Jeschke J. Stabilization of microvascular pedicles in intricate locations using fibrin glue. Microsurgery. 2008. 28: 509-13
9. Wang KC, Chen YL, Lin SL. Fibrin-based tissue glue for the prevention of kinking at sites of microvascular anastomoses. Br J Oral Maxillofac Surg. 2014. 52: 477-8
10. Yuan JY, Durward QJ, Pary JK, Vasgaard JE, Coggins PK. Use of duplex ultrasonography for identification and patch repair of kinking stenosis after carotid endarterectomy: A single-surgeon retrospective experience. World Neurosurg. 2014. 81: 334-43

