

- Department of Neurosurgery, Instituto Nacional de Neurologia y Neurocirugia, Mexico City, Mexico,
- Department of Neurology and Neurosurgery, McGill University, Montreal, Quebec, Canada.
- Division of Neurosurgery, Centre Hospitalier Saint-Justine, Montreal, Quebec, Canada.
Correspondence Address:
Michel G. Mondragon-Soto, Department of Neurosurgery, Instituto Nacional de Neurologia y Neurocirugia, Mexico City, Mexico.
DOI:10.25259/SNI_636_2021
Copyright: © 2022 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Michel Gustavo Mondragon-Soto1, Lior Elkaim2, Alexander G. Weil3. Transient ventriculoperitoneal shunt malfunction in a pediatric patient: An illustrative case. 05-Jan-2022;13:6
How to cite this URL: Michel Gustavo Mondragon-Soto1, Lior Elkaim2, Alexander G. Weil3. Transient ventriculoperitoneal shunt malfunction in a pediatric patient: An illustrative case. 05-Jan-2022;13:6. Available from: https://surgicalneurologyint.com/surgicalint-articles/11325/
Date of Submission
25-Jun-2021
Date of Acceptance
20-Sep-2021
Date of Web Publication
05-Jan-2022
Abstract
Background: Ventriculoperitoneal shunt (VPS), the mainstay of the treatment for hydrocephalus, is associated with relatively high revision rates. Transient hydrocephalus due to intermittent VPS obstruction should be recognized as a cause of VPS malfunction. While transient VPS dysfunction is well-recognized complication, there is a relative paucity of well-documented cases in the literature.
Case Description: We present the case of a 4-year-old boy with a history of vascular malformation and hydrocephalus secondary to intraventricular hemorrhage. The patient presented with transient, self-resolving hydrocephalus (without intervention), as documented by clinical and radiological findings.
Conclusion: Transient hydrocephalus due to intermittent VPS dysfunction in children is a rare entity, but it should be suspected in certain patients with VPS presenting with transient or self-improving symptoms.
Keywords: Choroid plexus, Hydrocephalus, Pediatric, Shunt malfunction
BACKGROUND
Hydrocephalus affects both pediatric and adult populations, with an estimated prevalence in the general populations of between 1.0% and 1.5%.[
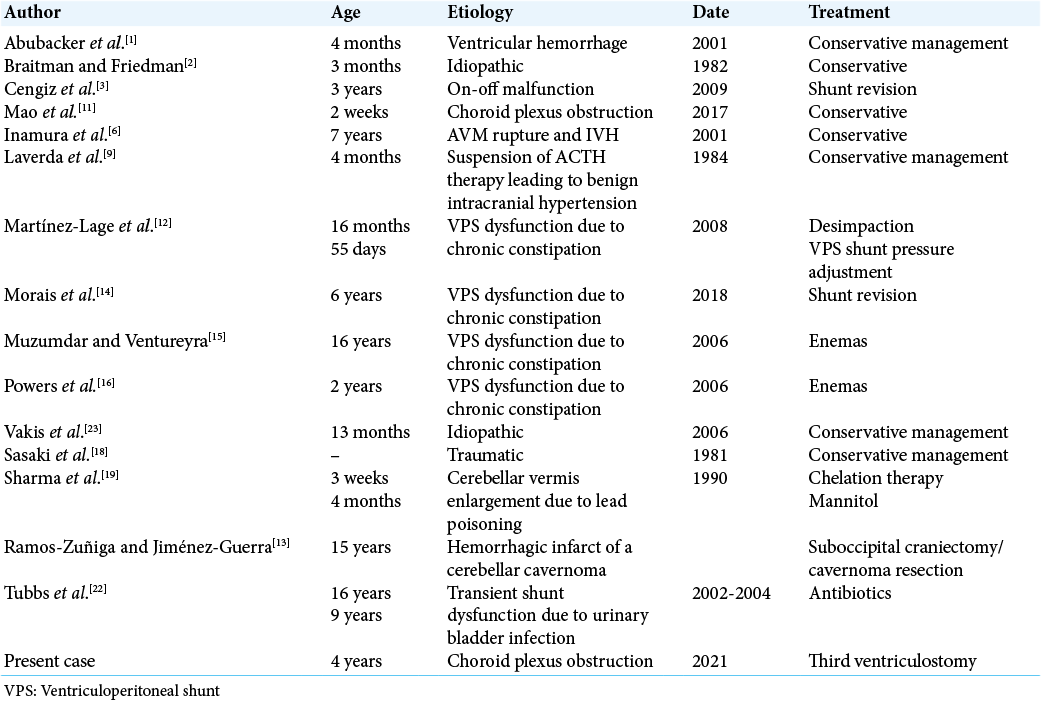
There are, to the best of our knowledge, 15 available case reports describing transient hydrocephalus in pediatric patients. Of these, only four represent patients with ventriculoperitoneal shunt (VPS) dysfunctions; other suspected etiologies include subarachnoid hemorrhage and intraventricular clots,[
In this report, we provide radiographic evidence on computed tomography (CT) and magnetic resonance imaging (MRI) of spontaneously resolving hydrocephalus secondary to suspected VPS dysfunction in a 4-year-old boy.
CASE DESCRIPTION
A 4-year-old boy presented to the Emergency room with recurrent episodes of vomiting. He had a prior history of embolized Vein of Galen malformation (treated at the age of 3 months) complicated by intraventricular hemorrhage and hydrocephalus which was treated with a VPS (age of 3 months). Over a 6-month period, he was hospitalized on four separate occasions for transient episodes of intractable vomiting, lasting on average <1 day. On his third hospitalization, a brain MRI [
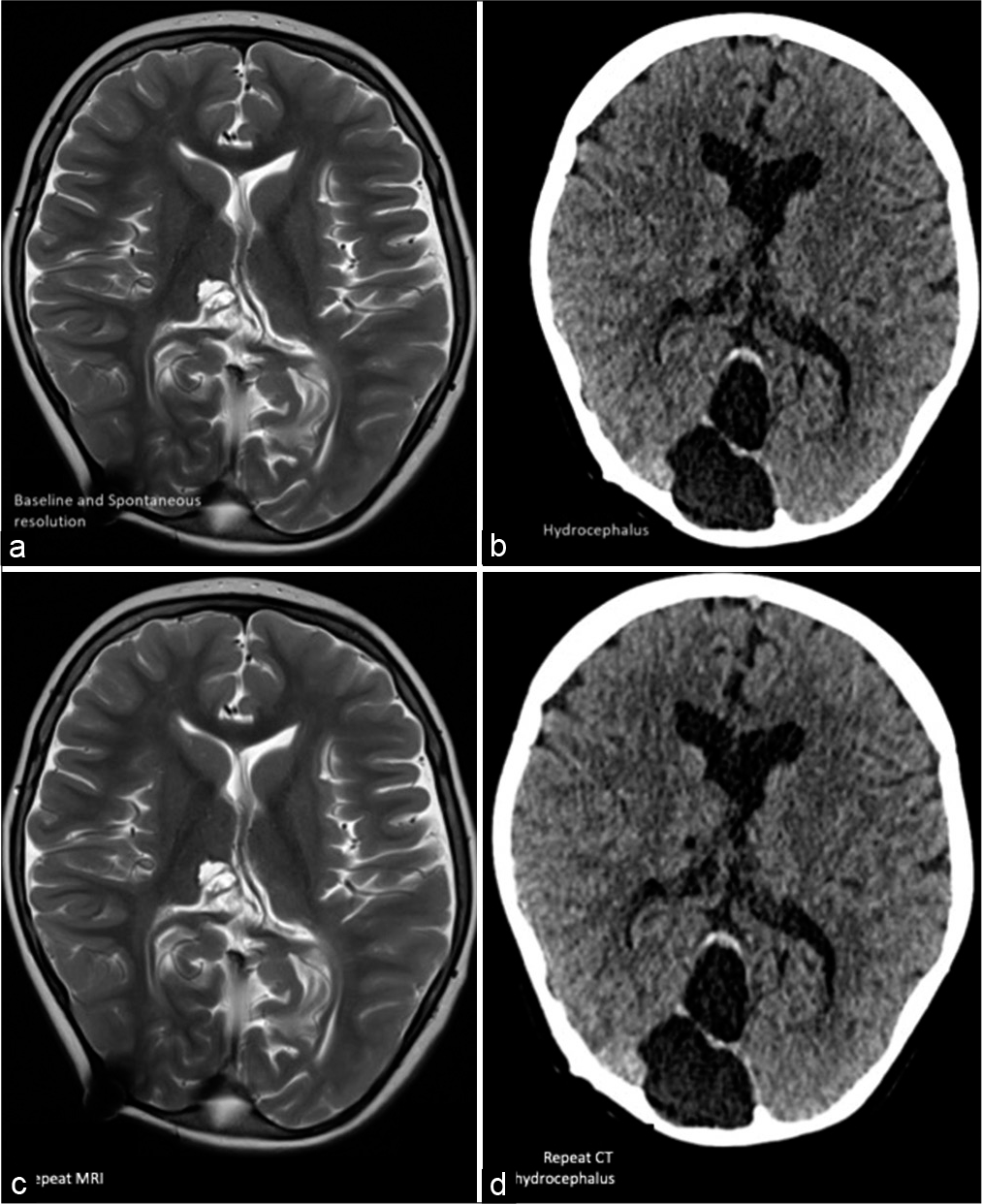
Figure 1:
(a) Baseline noncontrast axial T2 magnetic resonance imaging (MRI) demonstrating baseline ventricle size. (b) Noncontrast axial computed tomography (CT) in a 4-year-old boy with known ventriculoperitoneal shunt demonstrating acute hydrocephalus and increased ventricle size when compared with his baseline. (c) Repeat MRI on the morning of the scheduled OR demonstrating spontaneous resolution of hydrocephalus coinciding with symptomatic improvement. (d) Noncontrast axial CT performed a few weeks later demonstrating acute hydrocephalus.
DISCUSSION
Transient hydrocephalus has been described in pediatric patients with several proposed mechanisms, including intraventricular hemorrhage, suspension of ACTH therapy, carbon monoxide suspension, as well as other unknown etiologies.[
This case report is unique in that the 4-year-old boy already had a VP shunt in place. The transient hydrocephalus was most likely due to transient shunt dysfunction. The on-off shunt failure, as mentioned by Cengiz et al.,[
It is also possible that the catheter could transiently have been obstructed by blood cells or a heap of proteins in the CSF. One review analyzed patients after VP shunt insertion (15-year follow-up); here, 84% of patients required a revision, with catheter occlusion being the primary reason for VPS revision.[
CONCLUSION
Although transient hydrocephalus due to VPS dysfunction in children is rare, it should be suspected in certain patients with a VPS shunt presenting with transient or improving symptoms.
Treatment may range from conservative medical management to surgical intervention and shunt revision. Thorough workup and careful monitoring of patient status are important to guide surgical decision-making in patients suffering from suspected transient VPS malfunction.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Abubacker M, Bosma JJ, Mallucci CL, May PL. Spontaneous resolution of acute obstructive hydrocephalus in the neonate. Childs Nerv Syst. 2001. 17: 182-4
2. Braitman RE, Friedman M. Spontaneous resolution of acute hydrocephalus. Clin Pediatr (Phila). 1982. 21: 757-8
3. Cengiz C, Aydın K, Kocabiçak E. On-off malfunction in a pediatric shunt: A case report. J Exp Clin Med. 2009. 26: 142-4
4. Erol FS, Ozturk S, Akgun B, Kaplan M. Ventriculoperitoneal shunt malfunction caused by fractures and disconnections over 10 years of follow-up. Childs Nerv Syst. 2017. 33: 475-81
5. Goeser CD, McLeary MS, Young LW. Diagnostic imaging of ventriculoperitoneal shunt malfunctions and complications. Radiographics. 1998. 18: 635-51
6. Inamura T, Kawamura T, Inoha S, Nakamizo A, Fukui M. Resolving obstructive hydrocephalus from AVM. J Clin Neurosci. 2001. 8: 569-70
7. Jergović I, Budinčević H, Planjar-Prvan M, Bielen I. Transient obstructive hydrocephalus in patients with intracerebral hemorrhage: Report of two cases. Acta Clin Croat. 2016. 55: 497-500
8. Klarica M, Oresković D, Bozić B, Vukić M, Butković V, Bulat M. New experimental model of acute aqueductal blockage in cats: Effects on cerebrospinal fluid pressure and the size of brain ventricles. Neuroscience. 2009. 158: 1397-405
9. Laverda AM, Casara G, Battistella PA, Drigo P. Acute-onset transient hydrocephalus after suspension of ACTH therapy for infantile spasms: A case report. Ital J Neurol Sci. 1984. 5: 219-22
10. Lusis EA, Vellimana AK, Ray WZ, Chicoine MR, Jost SC. Transient obstructive hydrocephalus due to intraventricular hemorrhage: A case report and review of literature. J Clin Neurol. 2013. 9: 1925
11. Mao G, Agarwal N, Zuccoli G, Tyler-Kabara EC. Intermittent entrapment of choroid plexus in ventricular catheter. Interdiscip Neurosurg. 2017. 9: 17-9
12. Martínez-Lage JF, Martos-Tello JM, Ros-de-San Pedro J, Almagro MJ. Severe constipation: An under-appreciated cause of VP shunt malfunction: A case-based update. Childs Nerv Syst. 2008. 24: 431-5
13. Morais BA, Cardeal DD, Andrade FG, Paiva WS, Matushita H, Teixeira MJ. Reversible ventriculoperitoneal shunt dysfunction and chronic constipation: Case report. J Neurosurg Pediatr. 2018. 22: 147-50
14. Muzumdar D, Ventureyra EC. Transient ventriculoperitoneal shunt malfunction after chronic constipation: Case report and review of literature. Childs Nerv Syst. 2007. 23: 455-8
15. Powers CJ, George T, Fuchs HE. Constipation as a reversible cause of ventriculoperitoneal shunt failure. Report of two cases. J Neurosurg. 2006. 105: 227-30
16. Prabhu SS, Sharma RR, Gurusinghe NT, Parekh HC. Acute transient hydrocephalus in carbon monoxide poisoning: A case report. J Neurol Neurosurg Psychiatry. 1993. 56: 567-8
17. Ramos-Zuñiga R, Jiménez-Guerra R. Rational management of transient obstructive hydrocephalus secondary to a cerebellar infarct. Minim Invasive Neurosurg. 2006. 49: 302-4
18. Sasaki O, Furusawa Y, Takahara Y. Transient obstructive hydrocephalus of an infant following mild head injury (author’s transl). No Shinkei Geka. 1981. 9: 407-9
19. Sharma RR, Chandy MJ, Lad SD. Transient hydrocephalus and acute lead encephalopathy in neonates and infants. Report of two cases. Br J Neurosurg. 1990. 4: 141-5
20. Sivaganesan A, Krishnamurthy R, Sahni D, Viswanathan C. Neuroimaging of ventriculoperitoneal shunt complications in children. Pediatr Radiol. 2012. 42: 1029-46
21. Stone JJ, Walker CT, Jacobson M, Phillips V, Silberstein HJ. Revision rate of pediatric ventriculoperitoneal shunts after 15 years. J Neurosurg Pediatr. 2013. 11: 15-9
22. Tubbs RS, Wellons JC, Blount JP, Oakes WJ. Transient ventriculoperitoneal shunt dysfunction in children with myelodysplasia and urinary bladder infection. Report of three cases. J Neurosurg. 2005. 102: 221-3
23. Vakis AF, Karabetsos DA, Koutentakis DI, Flouris G, Fasoulaki M. Transient acute obstructive hydrocephalus of unknown origin in a 13-month-old infant. Eur J Paediatr Neurol. 2006. 10: 197-201

