

- Department of Neurosurgery, AIIMS Raipur, Tatibandh, Raipur, Chhattisgarh, India
- Department of Anaesthesiology AIIMS Raipur, Tatibandh, Raipur, Chhattisgarh, India
- Department of Radiology, AIIMS Raipur, Tatibandh, Raipur, Chhattisgarh, India
- Department of Pediatric Endocrinology, Bai Jerbai Wadia Hospital for Children, Parel, Mumbai, Maharashtra, India.
Correspondence Address:
Charandeep Singh Gandhoke
Department of Pediatric Endocrinology, Bai Jerbai Wadia Hospital for Children, Parel, Mumbai, Maharashtra, India.
DOI:10.25259/SNI_142_2020
Copyright: © 2020 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Gandhoke CS1, Gupta SK1, Sharma AK1, Ayalasomayajula S2, Sinha M2, Pati SK3, Syal SK4. Triplomyelia in a case of diastematomyelia: A new entity. Surg Neurol Int 08-Oct-2020;11:324
How to cite this URL: Gandhoke CS1, Gupta SK1, Sharma AK1, Ayalasomayajula S2, Sinha M2, Pati SK3, Syal SK4. Triplomyelia in a case of diastematomyelia: A new entity. Surg Neurol Int 08-Oct-2020;11:324. Available from: https://surgicalneurologyint.com/surgicalint-articles/10311/
Date of Submission
31-Mar-2020
Date of Acceptance
18-Sep-2020
Date of Web Publication
08-Oct-2020
We report the case of a 6-year-old female child, 3rd child of a nonconsanguineous marriage, who presented with complaints of weakness of the right lower limb and deformity of the right foot since birth. She also complained of fever on and off, abdominal pain and dribbling of urine for 4 months. On examination, power in the right lower limb was 3/5 and all sensations in the right lower limb were decreased. She also had right foot congenital talipes equinovarus. Urine Routine/ Microscopy was suggestive of urinary tract infection. Urine Culture/Sensitivity showed the growth of Escherichia coli. Antibiotics were given according to culture sensitivity. Her radiology revealed kyphoscoliotic deformity with segmentation anomalies including hemivertebrae and bifid spine at multiple levels, low lying tethered spinal cord (up to the upper sacral level) with diastematomyelia [Type 1 Split cord malformation (SCM) with 2 dural tubes] with a bony spur at D12/L1 level with triplomyelia at D10 level (3 hemicords within a single dural tube) and small lipomyelomeningocele attached to the right hemicord at L4/L5 level [

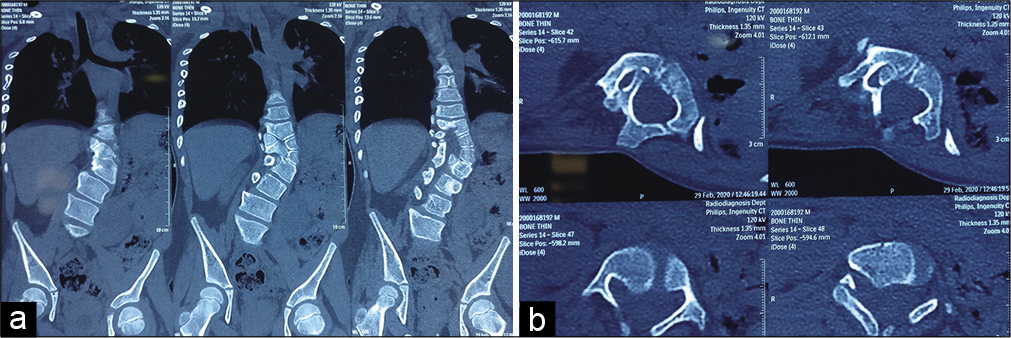
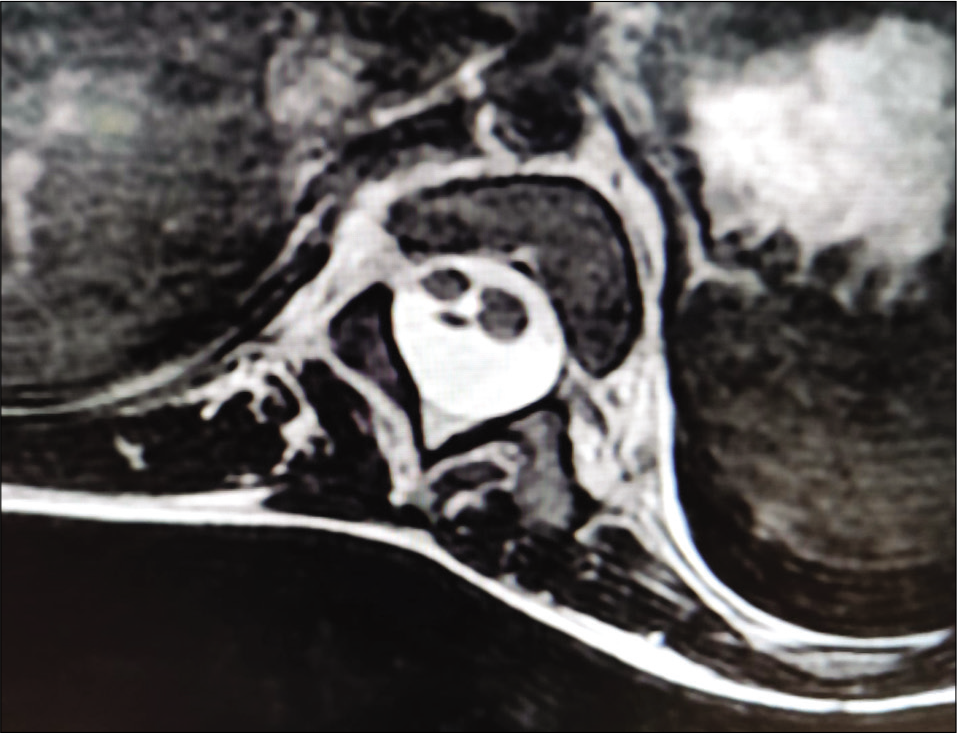
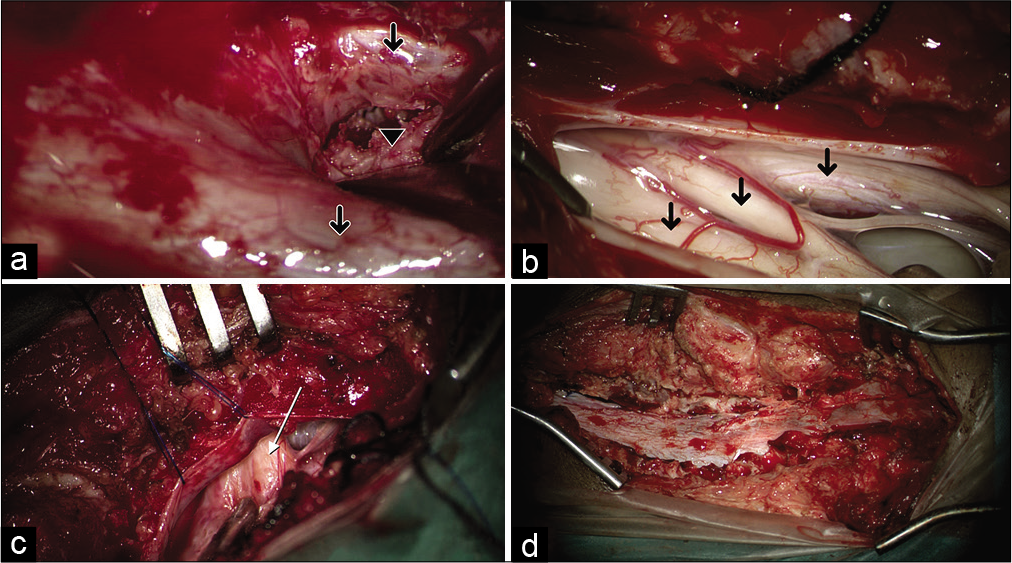
Figure 4:
Intraoperative photographs showing (a) diastematomyelia with two dural tubes (arrows), with a rigid bony septum in between (black arrowhead). (b) At D10 level, there was triplication of the spinal cord (arrows). The thicker left hemicord split again to form two smaller hemicords. Above and below this level, the left hemicord continued as one. (c) Lipomyelomeningocele attached to the right hemicord at L4/L5 level (arrow) (d) reconstitution of the dural tube into one at the end of the procedure.
SCM’s are of two types.[
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Pang D, Dias MS, Ahab-Barmada M. Split cord malformation: Part I: A unified theory of embryogenesis for double spinal cord malformations. Neurosurgery. 1992. 31: 451-80

