

- Department of Neurosurgery, Lithuanian University of Health Sciences, Kaunas, Lithuania
- Neuroscience Institute, Lithuanian University of Health Sciences, Kaunas, Lithuania
- Department of Psychiatry, Lithuanian University of Health Sciences, Kaunas, Lithuania
Correspondence Address:
Adomas Bunevicius
Department of Neurosurgery, Lithuanian University of Health Sciences, Kaunas, Lithuania
Neuroscience Institute, Lithuanian University of Health Sciences, Kaunas, Lithuania
DOI:10.4103/2152-7806.187489
Copyright: © 2016 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Bunevicius A, Cikotas P, Steibliene V, Deltuva VP, Tamsauskas A. Unruptured anterior communicating artery aneurysm presenting as depression: A case report and review of literature. Surg Neurol Int 01-Aug-2016;7:
How to cite this URL: Bunevicius A, Cikotas P, Steibliene V, Deltuva VP, Tamsauskas A. Unruptured anterior communicating artery aneurysm presenting as depression: A case report and review of literature. Surg Neurol Int 01-Aug-2016;7:. Available from: http://surgicalneurologyint.com/surgicalint_articles/unruptured-anterior-communicating-artery-aneurysm-presenting-depression-case-report-review-literature/
Abstract
Background:Intracranial aneurysms most commonly present following rupture causing subarachnoid hemorrhage. Mental disorders are common among patients with unruptured intracranial aneurysms and in aneurysmal subarachnoid hemorrhage survivors. However, to the best of our knowledge, there is no published report of unruptured intracranial aneurysm presenting as a mental disorder.
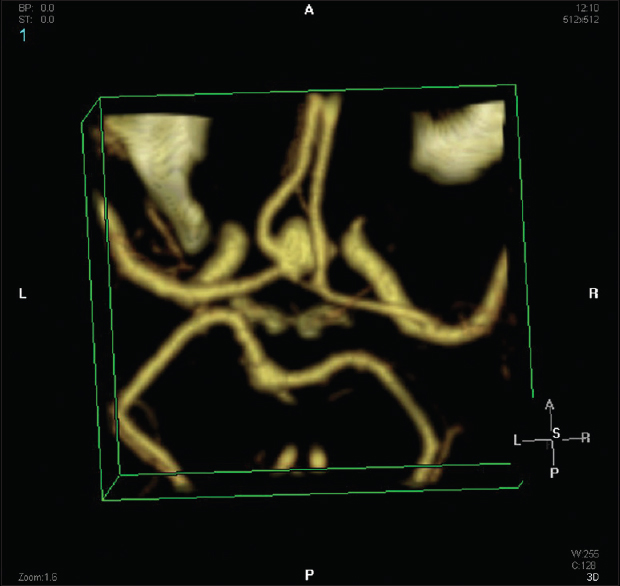
Case Description:A 69-year-old male without a past history of mental disorders and neurological symptoms presented with a 2-month history of anxiety, sadness, lack of pleasure in usual activities, fatigue, difficulties falling asleep and waking up early in the morning, reduced appetite, and weight loss. The patient was diagnosed with major depressive disorder and antidepressant treatment was initiated. Subsequent non-contrast computed tomography (CT) of the head demonstrated hypointense oval-shaped lesion within the projection of the anterior communicating artery. CT angiography confirmed the diagnosis of a 0.8 × 0.6 cm saccular aneurysm originating from the anterior communicating artery and anterior cerebral artery. The patient underwent microsurgical clipping of the aneurysm. On psychiatric assessment 1 month after the surgery, there were no signs of depressive disorder and antidepressive treatment was discontinued. On follow-up visit 1 year after the surgery, the patient did not have any mood symptoms.
Conclusions:The case indicates that organic brain lesions, including intracranial aneurysms, should be suspected in elderly patients presenting with their first episode of mental disorder.
Keywords: Intracranial aneurysm, major depressive episode, unruptured
INTRODUCTION
Aneurysm of intracranial arteries is rare but potentially fatal disorder affecting up to 5% of the general population.[
Rarely, intracranial aneurysms are diagnosed prior to rupture. The most common presenting signs and symptoms of unruptured intracranial aneurysms include headache, reduced visual acuity, double vision, and other cranial nerve neuropathies that are usually attributed to mass effect imposed by the aneurysm to nearby neural structures.[
CASE REPORT
Mr. G is a 69-year-old male who presented to his general practitioner with a 2-month history of anxiety, sadness, lack of pleasure in usual activities, fatigue, difficulties falling asleep and waking up early in the morning, reduced appetite, and significant weight loss. He has been working as a transport manager but had retired 1 month prior to presentation due to his current health problems. He was living alone in the countryside. The patient denied a past history of psychiatric or somatic disorders and was not taking any medication at the time of presentation. Physical examination revealed no abnormalities. Routine blood work that included clinical blood count and blood chemistry was evident for dyslipidemia.
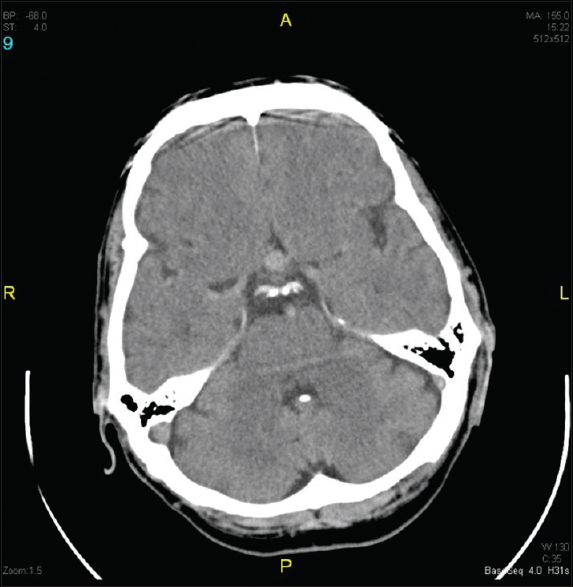
The patient was referred for neurology and psychiatry consultations. On psychiatric interview, the patient was alert, oriented, and was noted to have symptoms of psychomotor retardation, tearfulness, depressed mood, feelings of worthlessness, and pessimistic thoughts about the future. The patient denied suicidal thoughts. Neuropsychological testing demonstrated mild cognitive impairment due to concentration difficulties, and moderately severe depressive symptoms as well as mild anxiety symptoms. The patient's symptoms were mostly consistent with major depressive episode, and antidepressant treatment with mirtazapine 15 mg once daily was initiated. Neurological examination did not reveal any cranial nerve deficits. Non-contrast computed tomography (CT) of the head was ordered to rule out organic brain lesions. Rather unexpectedly, non-contrast head CT demonstrated hypointense oval-shaped lesion of 0.9 cm in diameter within the projection of the anterior communicating artery that was mostly consistent with a saccular aneurysm [
DISCUSSION
The current case report presents an uncommon presentation of an unruptured intracranial aneurysm as major depressive episode in an otherwise asymptomatic elderly patient without a past history of psychiatric disorders.
Possible biological mechanisms underlying the association between depressive symptoms and anterior communicating artery aneurysm cannot be discerned from the present case. Anterior communicating artery lies beneath the frontal lobes in the anterior aspect of the limbic system and connects two anterior cerebral arteries that provide major oxygenated blood supply to medial the portions of the frontal and parietal lobes and to the limbic system. It is well-described that structural abnormalities and organic lesions within the frontal lobe and limbic system can produce depressive symptoms.[
On the other hand, it is also possible that the patient had two unrelated conditions. However, it should be noted that the patient's presentation was not typical because depression usually manifests at a younger age and the patient denied a past history of psychiatric disorders. From a clinical perspective, the present case illustrates that careful neurologic and radiologic evaluation should be performed in middle-aged and elderly patients presenting with their first episode of psychiatric disorder. Detailed radiological investigation should be considered to rule out organic brain lesions. In the present case, an aneurysm was detected on non-contrast head CT scan. Low cost and short testing timing are the most important advantages of non-contrast head CT scan making it the most commonly employed imaging modality in routine clinical settings for initial screening purposes of patients with suspected organic brain lesions. Non-contrast CT scan can reliably detect certain brain tumors, hydrocephalus, and intracranial bleeding, such as SAH; however, it should not be used for intracranial aneurysm screening purposes. Magnetic resonance angiography (MRA) and CTA are recommended as reasonable diagnostic imaging modalities for intracranial aneurysm screening in asymptomatic patients.[
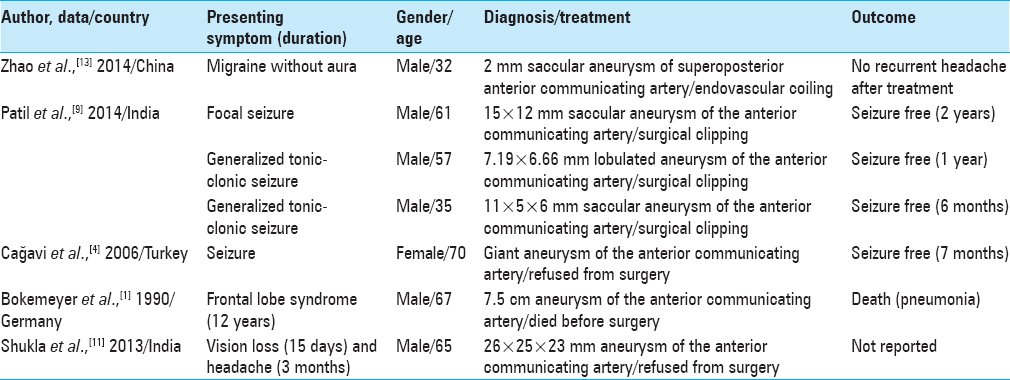
Aneurysm rupture causing SAH-associated symptoms remains the most common presentation of intracranial aneurysms. Unruptured intracranial aneurysms usually present with headache, reduced visual acuity, double vision, and other cranial nerve neuropathies that are usually caused by mass effect imposed by an aneurysm to nearby neural structures. However, it should be remembered that rarely unruptured intracranial aneurysms can cause other neurologic and neuropsychiatric symptoms and/or disorders. Other previously described unusual presentations of unruptured intracranial aneurysms include migraine without aura,[
CONCLUSION
We describe an uncommon association between depressive disorder and unruptured intracranial artery aneurysm in an elderly patient without a past history of psychiatric disorder. The case illustrates that elderly patients presenting with the first episode of psychiatric disorder should be carefully evaluated for underlying intracranial pathology, including unruptured aneurysm of intracranial arteries.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Bokemeyer C, Frank B, Brandis A, Weinrich W. Giant aneurysm causing frontal lobe syndrome. J Neurol. 1990. 237: 47-50
2. Brisman JL, Song JK, Newell DW. Cerebral aneurysms. N Eng J Med. 2006. 355: 928-39
3. Bunevicius A, Deltuva VP, Deltuviene D, Tamasauskas A, Bunevicius R. Brain lesions manifesting as psychiatric disorders: Eight cases. CNS spectr. 2008. 13: 950-8
4. Cağavi F, Kalayci M, Unal A, Atasoy HT, Cagavi Z, Acikgoz B. Giant unruptured anterior communicating artery aneurysm presenting with seizure. J Clin Neurosci. 2006. 13: 390-4
5. Friedman JA, Piepgras DG, Pichelmann MA, Hansen KK, Brown RD, Wiebers DO. Small cerebral aneurysms presenting with symptoms other than rupture. Neurology. 2001. 57: 1212-6
6. Johnston SC, Selvin S, Gress DR. The burden, trends, and demographics of mortality from subarachnoid hemorrhage. Neurology. 1998. 50: 1413-8
7. King JT, Kassam AB, Yonas H, Horowitz MB, Roberts MS. Mental health, anxiety, and depression in patients with cerebral aneurysms. J Neurosurg. 2005. 103: 636-41
8. Kobayashi H, Hayashi M, Kawano H, Handa Y, Kabuto M, Ishii Y. Magnetic resonance imaging of embolism from intracranial aneurysms. Surg Neurol. 1989. 32: 225-30
9. Patil A, Menon GR, Nair S. Unruptured anterior communicating artery aneurysms presenting with seizure: Report of three cases and review of literature. Asian J Neurosurg. 2013. 8: 164-
10. Sexton CE, Mackay CE, Ebmeier KP. A systematic review and meta-analysis of magnetic resonance imaging studies in late-life depression. Am J Geriatr Psychiatry. 2013. 21: 184-95
11. Shukla DP, Bhat DI, Devi BI. Anterior communicating artery aneurysm presenting with vision loss. J Neurosci Rural Pract. 2013. 4: 305-7
12. Wiebers DO, Whisnant JP, Huston J, Meissner I, Brown RD, Piepgras DG. Unruptured intracranial aneurysms: Natural history, clinical outcome, and risks of surgical and endovascular treatment. Lancet. 2003. 362: 103-10
13. Zhao M, Liu CS, Xu XY, Xiao YP, Fang C. Unruptured saccular aneurysm presenting migraine. Genet Mol Res. 2014. 13: 4046-9

