

- Pars Advanced and Minimally Invasive Medical Manners Research Center, Pars Hospital, Iran University of Medical Sciences, Tehran, Iran.
DOI:10.25259/SNI-308-2019
Copyright: © 2019 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Abolfazl Rahimizadeh, Zahed Malekmohammadi, Mona Karimi, Ava Rahimizadeh, Naser Asgari. Unstable os odontoideum contributing to cervical myelopathy and obstructive sleep apnea. 28-Jun-2019;10:125
How to cite this URL: Abolfazl Rahimizadeh, Zahed Malekmohammadi, Mona Karimi, Ava Rahimizadeh, Naser Asgari. Unstable os odontoideum contributing to cervical myelopathy and obstructive sleep apnea. 28-Jun-2019;10:125. Available from: http://surgicalneurologyint.com/surgicalint-articles/9437/
Date of Submission
14-May-2019
Date of Acceptance
27-May-2019
Date of Web Publication
28-Jun-2019
Abstract
Background: Sleep apnea is characterized by repetitive cessation of breathing during sleep. It may be attributed to obstructive, central, or mixed pathologies close to the upper airway resulting in a decreased diameter of the oropharyngeal tract.
Case Description: A 36-year-old male with progressive cervicomedullary myelopathy/quadriparesis exhibited obstructive sleep apnea (OSA) attributed to an anteriorly displaced os odontoideum (OO). Atlantoaxial screw-rod stabilization resulted in improvement of both neurological function and OSA.
Conclusion: A symptomatic unstable OO may contribute to suboccipital pain, progressive quadriparesis, vertebrobasilar insufficiency, and OSA. Appropriate operative intervention utilizing atlantoaxial screw-rod stabilization may help to resolve these deficits.
Keywords: Cervical myelopathy, Obstructive sleep apnea, OS odontoideum
INTRODUCTION
Obstructive sleep apnea (OSA) is defined by momentary, cyclical cessation in breathing that is not severe enough to cause significant arterial hypoxemia and/or hypercapnia.[
Os odontoideum (OO), a traumatic or congenital abnormality of the second cervical vertebrae, is characterized by a separate bony segment with a smooth circumferential margin.[
CASE REPORT
A 36-year-old male exhibited a progressive spastic quadriparesis (hyperactive reflexes, positive Hoffmann signs, and an equivocal plantar reflex bilaterally) of 6-month duration. He also had developed OSA over the past 2 years, documented by two overnight polysomnography studies.
Radiographic confirmation of OO
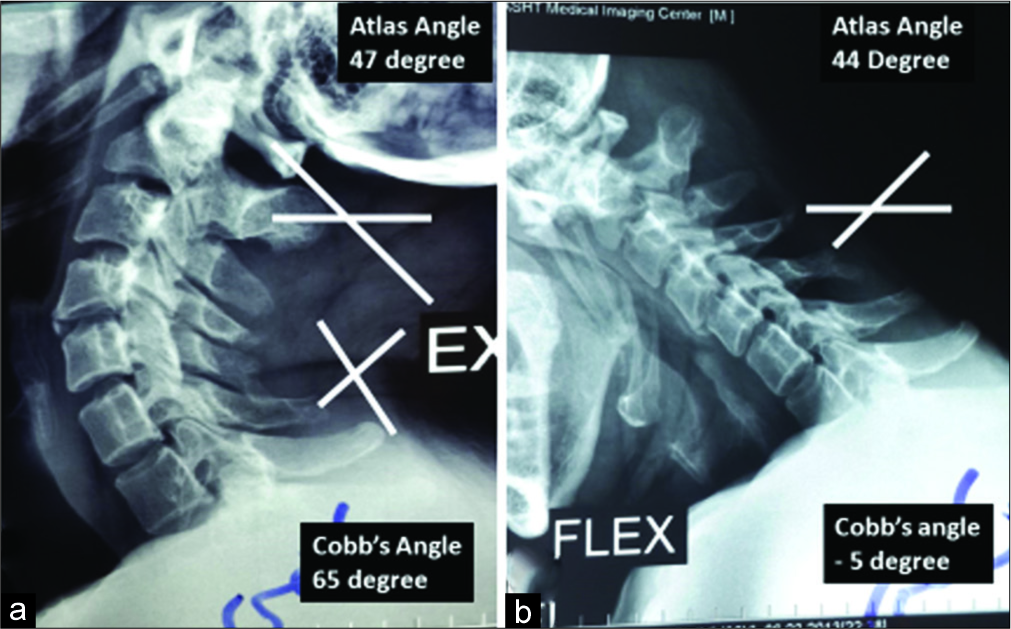
The dynamic lateral cervical X-rays showed a free-floating OO that compromised the oropharyngeal airway [
The cervical magnetic resonance imaging (MRI) showed atlantoaxial dislocation attributed to anterior displacement of the OO resulting in marked AP diameter canal narrowing at the cervicomedullary junction [

Figure 2:
(a) T1-weighted sagittal magnetic resonance imaging (MRI) of cervical spine shows an os odontoideum (OO) with atlantoaxial dislocation and narrowing of the cervicomedullary junction. The OO and atlas ring are engulfed in a soft tissue extending from os to axis. The posterior airway space is quite narrow in the MRI taken in neuter position (white dash). (b) T2-weighted sagittal MRI shows myelopathy at the cervicomedullary junction.
Computed tomography (CT) studies (coronal and sagittal images) also confirmed anterior displacement of the OO. The sagittal CT showed the characteristic jigsaw pattern [
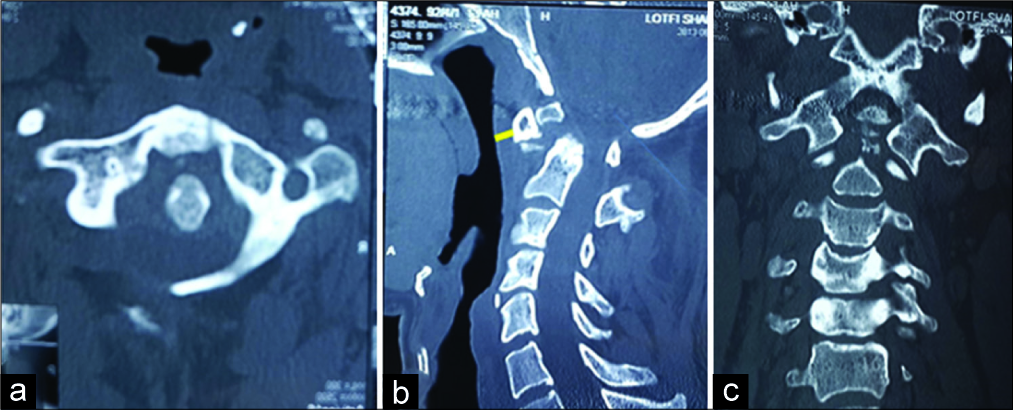
Figure 3:
Computed tomography scan of the cervical spine, (a) axial view shows atlantoaxial dislocation. (b) Reconstructed sagittal view shows displaced os odontoideum (OO) - atlas ring forward displacement in jigsaw pattern; note posterior airway space is very narrow with the neck in neuter position. (c) Reconstructed coronal view shows the OO.
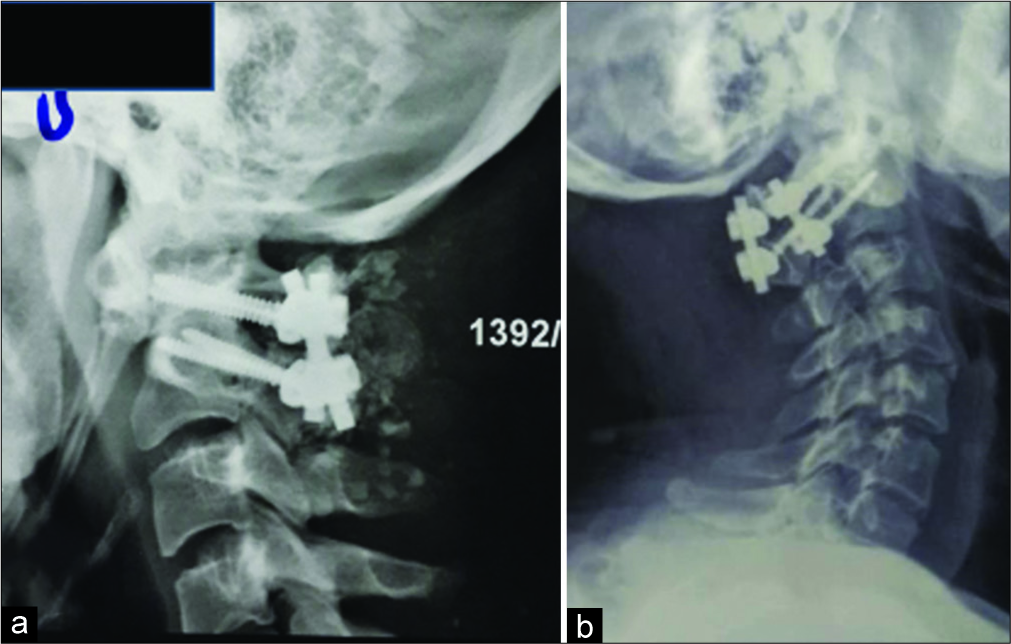
Surgery
The patient underwent a C1-C2 posterior fusion [
DISCUSSION
Frequency and etiology of OSA and rarity with OO
OSA is a relatively common but highly morbid condition that affects middle-aged adults (e.g., 9.1% of males and 4% of females).[
Surgery for OO
The surgical management of unstable OO requires C1-C2 reduction and fusion/fixation best achieved with the classic Harms technique.[
CONCLUSION
A symptomatic os odontoideum may contribute to suboccipital pain, progressive quadriparesis, vertebrobasilar insufficiency, and OSA. Appropriate operative intervention may help resolve these deficits.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patients have given their consent for their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Ataka H, Tanno T, Miyashita T, Isono S, Yamazaki M. Occipitocervical fusion has potential to improve sleep apnea in patients with rheumatoid arthritis and upper cervical lesions. Spine (Phila Pa 1976). 2010. 35: E971-5
2. Darakjian A, Darakjian AB, Chang ET, Camacho M. Refractory obstructive sleep apnea in a patient with diffuse idiopathic skeletal hyperostosis. Case Rep Otolaryngol. 2016. 2016: 4906863-
3. Douglas NJ, Polo O. Pathogenesis of obstructive sleep apnoea/ hypopnoea syndrome. Lancet. 1994. 344: 653-5
4. Epstein LJ, Kristo D, Strollo PJ, Friedman N, Malhotra A, Patil SP. Clinical guideline for the evaluation, management and long-term care of obstructive sleep apnea in adults. J Clin Sleep Med. 2009. 5: 263-76
5. Eyigor H, Selcuk OT, Osma U, Koca R, Yilmaz MD. Cervical osteophytes: A rare cause of obstructive sleep apnea. J Craniofac Surg. 2012. 23: e444-6
6. Hughes TA, Wiles CM, Lawrie BW, Smith AP. Case report: Dysphagia and sleep apnoea associated with cervical osteophytes due to diffuse idiopathic skeletal hyperostosis (DISH). J Neurol Neurosurg Psychiatry. 1994. 57: 384-
7. Kawaguchi Y, Iida M, Seki S, Nakano M, Yasuda T, Asanuma Y. Os odontoideum with cervical mylopathy due to posterior subluxation of C1 presenting sleep apnea. J Orthop Sci. 2011. 16: 329-33
8. Khan A, Than KD, Chen KS, Wang AC, La Marca F, Park P. Sleep apnea and cervical spine pathology. Eur Spine J. 2014. 23: 641-7
9. Rahimizadeh A, Rahimizadeh A. Os odontoideum: A review article. Orthop Res Traumatol. 2016. 1: 33-55
10. Rahimizadeh A, Soufiani HF, Hassani V, Rahimizadeh A. Atlantoaxial subluxation due to an os odontoideum in an achondroplastic adult: Report of a case and review of the literature. Case Rep Orthop. 2015. 2015: 142586-
11. Rahimizadeh A, Taginedjadi O, Rahimizadeh S, Saghri M, Rahimizadeh A. Respiratory distress and dysphagia secondary to diffuse idiopathic skeletal hyperostosis: Case report and review. World Spinal Column J. 2013. 4: 18-24
12. Rahimizadeh A, Williamson WL, Rahimizadeh S, Amirzadeh M. Atlantoaxial subluxation secondary to unstable os odontoideum in a patient with arrested hydrocephalus due to congenital aqueductal stenosis: A Case report. Int J Spine Surg. 2018. 12: 549-56
13. Wang V, Chou D. Anterior C1-2 osteochondroma presenting with dysphagia and sleep apnea. J Clin Neurosci. 2009. 16: 581-2
14. White DP. Pathogenesis of obstructive and central sleep apnea. Am J Respir Crit Care Med. 2005. 172: 1363-70
15. Yoshida T, Matsuda H, Horiuchi C, Taguchi T, Nagao J, Aota Y. A case of osteochondroma of the atlas causing obstructive sleep apnea syndrome. Acta Otolaryngol. 2006. 126: 445-8
16. Yosunkaya S, Pekcan S. Complex sleep apnea syndrome in a child with chiari malformation Type 1. Turk J Pediatr. 2013. 55: 107-11

