

- Department of Neurosurgery, Graduate School of Medical and Dental Sciences, Kagoshima University, Kagoshima, Japan
- Department of Neurosurgery, Atsuchi Neurosurgical Hospital, Kagoshima, Japan
Correspondence Address:
Takashi Kawahara
Department of Neurosurgery, Graduate School of Medical and Dental Sciences, Kagoshima University, Kagoshima, Japan
DOI:10.4103/2152-7806.183486
Copyright: © 2016 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Kawahara T, Oyoshi T, Atsuchi M, Takasaki K, Arita K. Use of the guidewire for repositioning displaced spinal catheter during lumboperitoneal shunt placement. Surg Neurol Int 06-Jun-2016;7:63
How to cite this URL: Kawahara T, Oyoshi T, Atsuchi M, Takasaki K, Arita K. Use of the guidewire for repositioning displaced spinal catheter during lumboperitoneal shunt placement. Surg Neurol Int 06-Jun-2016;7:63. Available from: http://surgicalneurologyint.com/surgicalint_articles/use-of-the-guidewire-for-repositioning-displaced-spinal-catheter-during-lumboperitoneal-shunt-placement/
Abstract
Background:During lumboperitoneal shunt operation, we may inadvertently pull and displace the spinal catheter after the catheter placement into the spinal canal. The authors introduce an easy and efficient technique for repositioning a prolapsed catheter into correct place.
Methods:After the confirmation of cerebrospinal fluid outflow from the end of the catheter, a guidewire for angiogram was gently inserted into the catheter until its tip reached the end of the catheter. The guidewire-inserted catheter was able to be pushed back manually and adequately placed in the spinal canal under the fluoroscope guidance.
Results:Three patients underwent repositioning using this “rescue wire technique” without complications.
Conclusion:This “rescue wire technique” is useful for repositioning of the displaced catheter into the spinal canal.
Keywords: Guidewire, lumboperitoneal shunt, spinal catheter
INTRODUCTION
After placement of spinal catheter into spinal canal in lumboperitoneal shunt (LPS) operation, we need several procedures such as removal of the Tuohy needle, connect the spinal catheter to the programmable valve, and subcutaneous placement of the abdominal catheter using a passer.[
SURGICAL TECHNIQUE
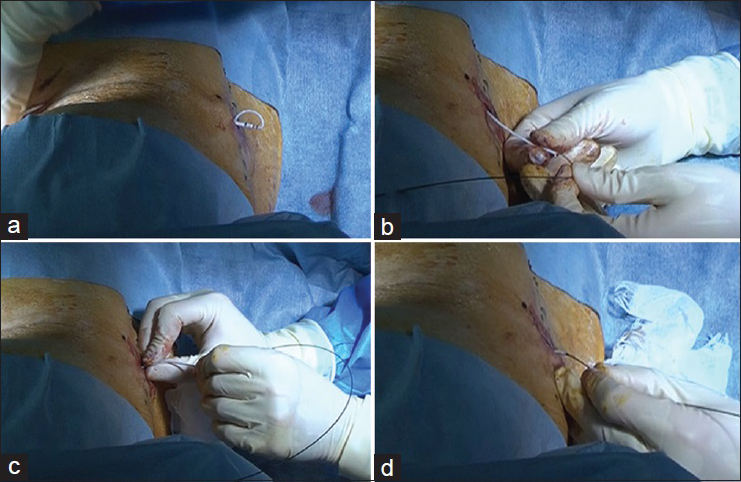
Distal end of the prolapsed spinal catheter is checked that the cerebrospinal fluid (CSF) flows out from the end of the catheter. After the spinal catheter has been connected to the programmable valve, it should be disconnected from the valve. A guidewire [
RESULTS
Three patients underwent repositioning using this “rescue wire technique.” In each case, the catheter was successfully replaced into the appropriate place. There were neither difficulties nor complications.
DISCUSSION
Once the spinal catheter is placed in the spinal canal with appropriate intrathecal length, Tuohy needle is removed from the back. After this step, prolapsed spinal catheter cannot be pushed back into the spinal canal due to softness of catheter. Before introducing this technique, we made another puncture using Tuohy needle for reinsertion of the spinal catheter.
The insertion of a guidewire into the catheter made the catheter maneuverable and could be pushed back. So far, in three patients, no spinal nerve injury has happened, probably because the inserted length of the guidewire is limited to the length of the catheter and the tip of guidewire is soft [
CONCLUSION
This simple method using guidewire under fluoroscope guidance is safe and effective for repositioning of the spinal catheter which accidentally prolapsed during LPS surgery.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Aoki N. Lumboperitoneal shunt: clinical applications, complications, and comparison with ventriculoperitoneal shunt. Neurosurgery. 1990. 26: 998-1003
2. Bloch O, McDermott MW. Lumboperitoneal shunts for the treatment of normal pressure hydrocephalus. J Clin Neurosci. 2012. 19: 1107-11
3. Wang VY, Barbaro NM, Lawton MT, Pitts L, Kunwar S, Parsa AT. Complications of lumboperitoneal shunts. Neurosurgery. 2007. 60: 1045-8
4. Yoshida S, Masunaga S, Hayase M, Oda Y. Migration of the shunt tube after lumboperitoneal shunt – Two case reports. Neurol Med Chir (Tokyo). 2000. 40: 594-6

