

- Department of Neurosurgery, Kouhoukai Takagi Hospital, Fukuoka, Japan
- Department of Neurosurgery, International University of Health and Welfare, School of Medicine, Narita City, Chiba, Japan
- Department of Neurosurgery, International University of Health and Welfare, Narita, Japan
- Department of Neurosurgery, Faculty of Medicine, Saga University, Saga, Japan.
Correspondence Address:
Tatsuya Tanaka, Department of Neurosurgery, International University of Health and Welfare, School of Medicine, Narita, City, Chiba, Japan.
DOI:10.25259/SNI_923_2023
Copyright: © 2024 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Yukinori Takase1, Tatsuya Tanaka2, Satoshi Anai1, May Pyae Kyaw1, Yuhei Michiwaki2, Hiroshi Itokawa2, Fumitaka Yamane3, Tatsuya Abe4, Akira Matsuno2. Usefulness of non-slip element percutaneous transluminal angioplasty scoring balloons in treating severe calcified lesions of the carotid artery for carotid artery stenting: A case report. 15-Mar-2024;15:91
How to cite this URL: Yukinori Takase1, Tatsuya Tanaka2, Satoshi Anai1, May Pyae Kyaw1, Yuhei Michiwaki2, Hiroshi Itokawa2, Fumitaka Yamane3, Tatsuya Abe4, Akira Matsuno2. Usefulness of non-slip element percutaneous transluminal angioplasty scoring balloons in treating severe calcified lesions of the carotid artery for carotid artery stenting: A case report. 15-Mar-2024;15:91. Available from: https://surgicalneurologyint.com/surgicalint-articles/12798/
Date of Submission
17-Nov-2023
Date of Acceptance
21-Feb-2024
Date of Web Publication
15-Mar-2024
Abstract
Background: Treatment of calcified lesions with conventional angioplasty balloons can be difficult due to insufficient lumen expansion, high dissection rates, and repeated revascularization. We report a case in which a scoring balloon was used in lesions resistant to angioplasty with a semi-compliant balloon.
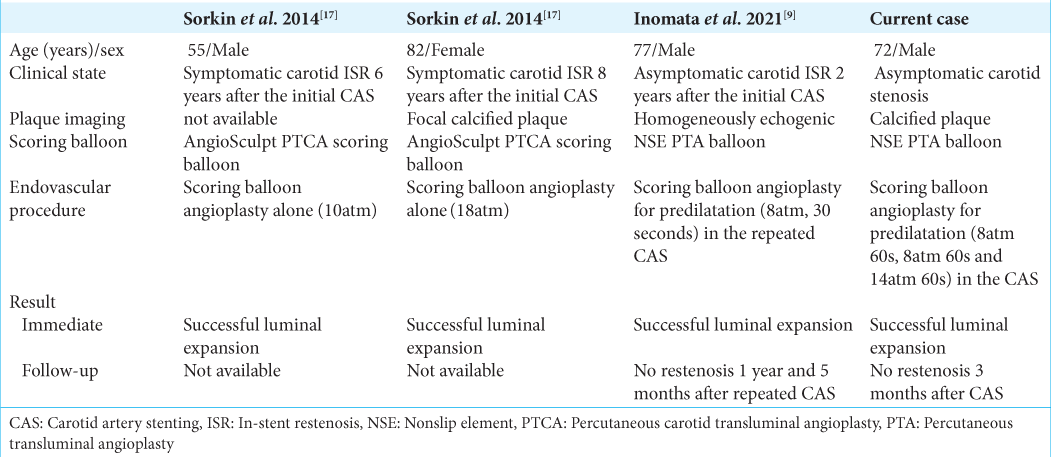
Case Description: A 72-year-old man presented with severe stenosis and a highly calcified lesion in the right cervical internal carotid artery. Right carotid artery stenting (CAS) was planned to prevent future ischemic stroke events. Conventional semi-compliant balloon angioplasty was unsuccessful. Three inflations of a non-slip element (NSE) percutaneous transluminal angioplasty (PTA) scoring balloon (Nipro, Osaka, Japan) successfully achieved CAS without complications.
Conclusion: This is the first report to describe the use of this scoring balloon in de novo carotid artery disease. NSE PTA scoring balloon catheters can be a useful option for refractory, highly calcified stenosis.
Keywords: Balloon angioplasty, Calcification, Carotid artery stenting, Endovascular treatment, Non-slip element balloon, Predilatation
INTRODUCTION
Carotid artery stenting (CAS) is increasingly used for treating carotid artery stenosis as an alternative to carotid endarterectomy for revascularization. Managing calcified lesions using traditional angioplasty balloons can pose challenges due to limited lumen dilation, elevated dissection risks, and the need for repeated revascularization.[
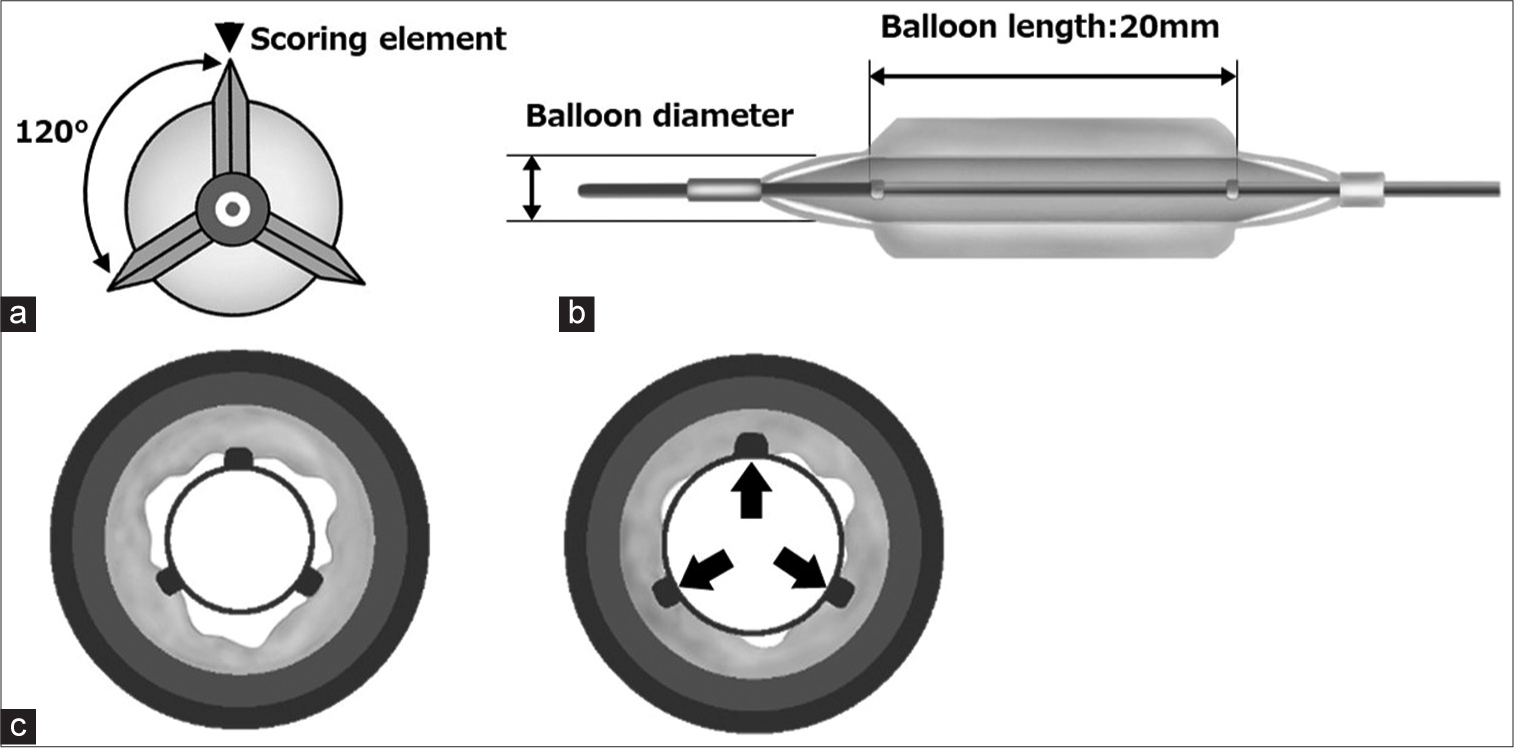
Figure 1:
Non-slip element percutaneous transluminal angioplasty (NSE PTA) balloon. (a) The NSE PTA balloon is a non-slip angioplasty catheter with three nylon scoring elements for controlled scoring of the vessel wall and reducing slippage during balloon inflation. (b) Stabilization of the balloon within the lesion during inflation. (c) Provision of an effective scoring effect through high concentrated force transmission (arrow).
Here, we describe the case of a patient with carotid calcified lesions who successfully underwent CAS with a scoring balloon and review the literature on carotid interventions with scoring balloons.
CASE DESCRIPTION
A 72-year-old man with a history of hypertension, diabetes mellitus, and cerebral infarction presented to our hospital with progressive left-sided hemiparesis four months previously. At the initial presentation, cranial magnetic resonance imaging/cranial and cervical magnetic resonance angiography revealed right cervical internal carotid artery (ICA) stenosis; moreover, acute and subacute infarctions in the right ICA territory were observed on diffusion-weighted image sequences [
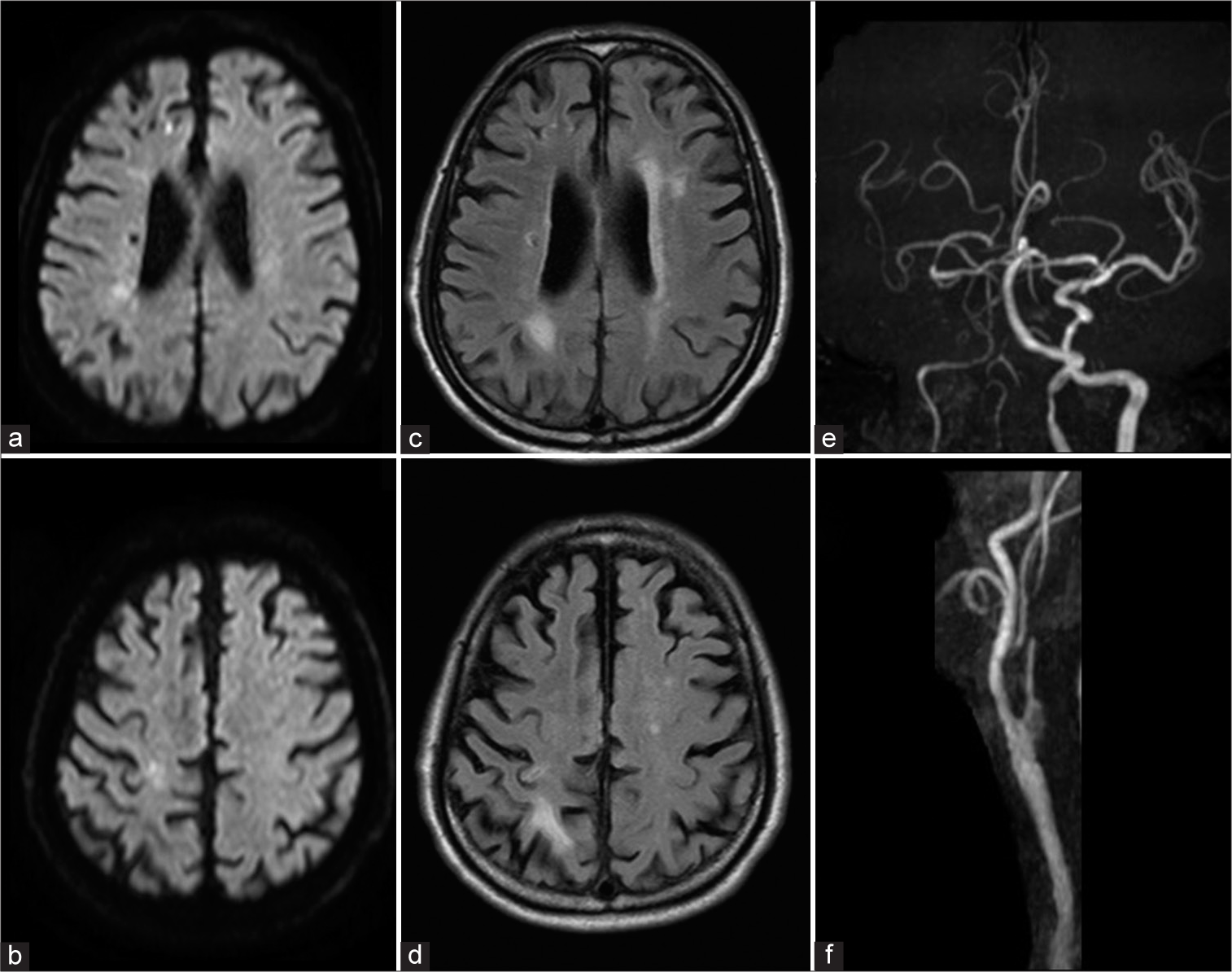
Figure 2:
(a and b) Initial magnetic resonance imaging, diffusion-weighted image, (c and d) fluid-attenuated inversion recovery image, and (e and f) magnetic resonance angiography showing acute and subacute infarcts in the territory of the right internal carotid artery (ICA) and right cervical ICA stenosis.

Figure 4:
Intraprocedural common carotid angiograms of the patient with severe calcified stenosis of the right carotid artery who underwent carotid artery stenting (CAS) with a non-slip element percutaneous transluminal angioplasty (NSE PTA) balloon. (a) A common carotid angiogram reveals severe stenosis (white arrow) of the right cervical internal carotid artery (ICA) (white arrow). (b) An NSE PTA balloon was placed in the cervical ICA, centered on the stenotic lesion, and used for pre-dilatation in the CAS. The NSE PTA balloon was inflated three times with Filter-Wire EZ underprotection. (c) Post-PTA shows mild improvement of the stenosis. (d) Placement of an 8 × 29 mm Carotid Wallstent Monorail. (e) Post-dilatation using a 4 mm × 40 mm SHIDEN balloon dilatation catheter. (f) Post-PTA showing the dilated stent. (g) A postprocedural common carotid angiogram reveals satisfactory revascularization.
Right CAS was planned to prevent future ischemic stroke events. The patient was treated with 100 mg aspirin and 200 mg cilostazol daily for four weeks before the procedure.
With the patient under local anesthesia, a 7-Fr long sheath was inserted into the right femoral artery, and a 7-Fr Optimo (Tokai Medical Products, Aichi, Japan) was delivered to the right common carotid artery. An activated clotting time of 250 seconds was maintained using intravenous heparin. A distal protection device (Filter-Wire EZ; Stryker, Fremont, California, USA) was inserted into the ICA. This device crossed the stenotic lesion after inflation of the guiding catheter balloon with proximal flow control. Attempts with a 3 mm × 40 mm SHIDEN balloon dilatation catheter (Kaneka, Osaka, Japan) and a 4 mm × 40 mm SHIDEN balloon dilatation catheter were unsuccessful despite inflation to a nominal pressure of 8 atm for 45 s. An 8 × 29 mm Carotid Wallstent Monorail (Boston Scientific, Natick, MA, USA) was inserted into the ICA and did not cross the stenotic lesion. Restenosis was thought to be caused by recoil. An NSE PTA balloon with three longitudinal nylon elements attached proximally and distally to the balloon component was used as a pre-dilatation step [
No postprocedural stroke events occurred [
DISCUSSION
In this case, a scoring balloon was used to successfully treat a highly calcified carotid artery stenosis lesion that could not be adequately dilated using the conventional technique.
High rates of carotid plaque calcification are associated with high rates of residual stenosis and restenosis.[
NSE PTA balloons are low-profile, semi-compliant scoring balloons with three triangular nylon elements that can score even a stiff plaque wall.[
To increase the luminal area during the initial procedure, a method that involves prolonged or multiple inflations of a scoring balloon has been reported.[
CONCLUSION
This is the first report to describe the use of a scoring balloon for de novo carotid artery disease. NSE PTA balloon catheters can be a useful option for refractory, highly calcified stenosis.
Ethical approval
The Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Journal or its management. The information contained in this article should not be considered to be medical advice; patients should consult their own physicians for advice as to their specific medical needs.
References
1. AbuRahma AF, DerDerian T, Hariri N, Adams E, AbuRahma J, Dean LS. Anatomical and technical predictors of perioperative clinical outcomes after carotid artery stenting. J Vasc Surg. 2017. 66: 423-2
2. Aoki J, Nakazawa G, Ando K, Nakamura S, Tobaru T, Sakurada M. Effect of combination of non-slip element balloon and drug-coating balloon for in-stent restenosis lesions (ELEGANT study). J Cardiol. 2019. 74: 436-42
3. Ashida K, Hayase T, Shinmura T. Efficacy of lacrosse NSE using the “leopard-crawl” technique on severely calcified lesions. J Invasive Cardiol. 2013. 25: 555-64
4. Castriota F, de Campos Martins EC, Setacci C, Manetti R, Khamis H, Spagnolo B. Cutting balloon angioplasty in percutaneous carotid interventions. J Endovasc Ther. 2008. 15: 655-62
5. Cotroneo AR, Pascali D, Iezzi R. Cutting balloon versus conventional balloon angioplasty in short femoropopliteal arterial stenoses. J Endovasc Ther. 2008. 15: 283-91
6. De Ribamar Costa J, Mintz GS, Carlier SG, Mehran R, Teirstein P, Sano K. Nonrandomized comparison of coronary stenting under intravascular ultrasound guidance of direct stenting without predilation versus conventional predilation with a semi-compliant balloon versus predilation with a new scoring balloon. Am J Cardiol. 2007. 100: 812-7
7. Giannopoulos S, Speziale F, Vadalà G, Soukas P, Kuhn BA, Stoltz CL. Intravascular lithotripsy for treatment of calcified lesions during carotid artery stenting. J Endovasc Ther. 2021. 28: 93-9
8. Grafmuller LE, Lehane DJ, Dohring CL, Zottola ZR, Mix DS, Newhall KA. Impact of calcified plaque volume on technical and 3-year outcomes after transcarotid artery revascularization. J Vasc Surg. 2023. 78: 150-7
9. Inomata Y, Hanaoka Y, Koyama JI, Suzuki Y, Fujii Y, Ogiwara T. Endovascular revascularization with a scoring balloon for carotid in-stent restenosis: Case report and literature review. Clin Neuroradiol. 2021. 31: 1199-204
10. Karashima E, Yoda S, Yasuda S, Kajiyama S, Ito H, Kaneko T. Usefulness of the “non-slip element” percutaneous transluminal angioplasty balloon in the treatment of femoropopliteal arterial lesions. J Endovasc Ther. 2020. 27: 102-8
11. Novitskaya E, Zin C, Chang N, Cory E, Chen P, D’Lima D. Creep of trabecular bone from the human proximal tibia. Mater Sci Eng C Mater Biol Appl. 2014. 40: 219-27
12. Otsuka Y, Koyama T, Imoto Y, Katsuki Y, Kawahara M, Nakamura K. Prolonged inflation technique using a scoring balloon for severe calcified lesion. Int Heart J. 2017. 58: 982-7
13. Poncyljusz W, Falkowski A, Safranow K, Rać M, Zawierucha D. Cuttingballoon angioplasty versus balloon angioplasty as treatment for short atherosclerotic lesions in the superficial femoral artery: Randomized controlled trial. Cardiovasc Intervent Radiol. 2013. 36: 1500-7
14. Scheinert D, Peeters P, Bosiers M, O’Sullivan G, Sultan S, Gershony G. Results of the multicenter first-in-man study of a novel scoring balloon catheter for the treatment of infra-popliteal peripheral arterial disease. Catheter Cardiovasc Interv. 2007. 70: 1034-9
15. Setacci F, Sirignano P, de Donato G, Chisci E, Galzerano G, Iacoponi F. Carotid highly-calcified de novo stenosis and cutting-balloon angioplasty: A tool to prevent haemodynamic depression?. J Cardiovasc Surg (Torino). 2009. 50: 357-64
16. Soga Y, Ando K. Effect of an NSE PTA balloon in experimental lesion models. Cardiovasc Interv Ther. 2018. 33: 35-9
17. Sorkin GC, Dumont TM, Eller JL, Mokin M, Hopkins LN, Snyder KV. Instent restenosis after carotid stenting: Treatment using an off-label cardiac scoring balloon. J Vasc Interv Neurol. 2014. 7: 29-34
18. Taguchi I, Kageyama M, Kanaya T, Abe S, Node K, Inoue T. Clinical significance of non-slip element balloon angioplasty for patients of coronary artery disease: A preliminary report. J Cardiol. 2014. 63: 19-23
19. Tanaka T, Michiwaki Y, Yamane F, Wakamiya T, Sashida R, Fujiwara R. Stent retriever angioplasty for acute atherosclerotic occlusion of internal carotid artery: A case report. Surg Neurol Int. 2022. 13: 482
20. Vadalà G, Galassi AR, Nerla R, Micari A. Shockwave intravascular lithoplasty for the treatment of calcified carotid artery stenosis: A very early single-center experience. Catheter Cardiovasc Interv. 2020. 96: E608-13

