

- Department of Neurosurgery, University of Arkansas for Medical Sciences, Little Rock, AR, USA
- Department of Radiology, University of Arkansas for Medical Sciences, Little Rock, AR, USA
Correspondence Address:
Noojan Kazemi
Department of Neurosurgery, University of Arkansas for Medical Sciences, Little Rock, AR, USA
DOI:10.4103/sni.sni_346_18
Copyright: © 2019 Surgical Neurology International This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.How to cite this article: Arunprasad Gunasekaran, Hamilton Newhart, Manoj Kumar, Noojan Kazemi. Utility of MRI neurography in neurofibromatosis type I: Case example and review of MRI neurography literature. 25-Jan-2019;10:12
How to cite this URL: Arunprasad Gunasekaran, Hamilton Newhart, Manoj Kumar, Noojan Kazemi. Utility of MRI neurography in neurofibromatosis type I: Case example and review of MRI neurography literature. 25-Jan-2019;10:12. Available from: http://surgicalneurologyint.com/surgicalint-articles/9194/
Date of Submission
08-Oct-2018
Date of Acceptance
20-Nov-2018
Date of Web Publication
25-Jan-2019
Abstract
Background:Neurofibromatosis is an autosomal dominant disorder of the nerves, resulting in café-au-lait spots, axillary freckling, macules, and neurofibromas throughout the nervous system. Diagnosis of this condition has in the past been mainly clinical, but the usage of magnetic resonance imaging neurography (MRN) is a new diagnostic modality. Here, we report on a case of neurofibromatosis type I (NF-1) that was diagnosed using MRN after a protracted clinical course.
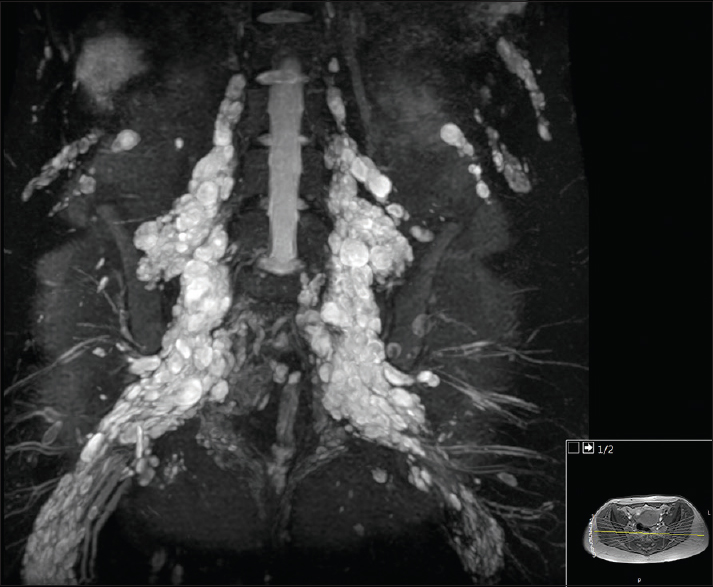
Case Description:A 23-year-old female presented with several months of worsening right upper and lower quadrant abdominal pain. The patient underwent computed tomography (CT) of the abdomen and pelvis demonstrating multiple neurofibromas involving the psoas muscle and mesentery of the lower abdomen. Subsequent total neuronal axis magnetic resonance imaging (MRI) using the neurography protocol (MRN) showed multiple neurofibromas in both the right brachial plexus and lumbar plexus.
Conclusion:We present a case of NF-1 that was diagnosed using MRN following a protracted clinical course. MRN is a diagnostic modality for NF-1 and other peripheral nerve disorders.
Keywords: Lumbar plexus, MRI neurography, neurofibromatosis type I
INTRODUCTION
Neurofibromatosis is an autosomal dominant disorder characterized by café-au-lait spots, axillary freckling macules, and neurofibromas scattered throughout the nervous system. While neurofibromatosis type I (NF-1) is typically diagnosed with genetic testing, it is often missed on clinical examination because of its variable expressivity. Here, we report on a patient with NF-1 who was diagnosed using magnetic resonance imaging neurography (MRN) after a protracted clinical course. MRN is a new useful diagnostic modality that can be used in patients at high suspicion for NF-1 and other peripheral nerve sheath tumors. It can also be used for preoperative surgical planning and postoperative surgical monitoring.
CASE ILLUSTRATION
A 23-year-old female presented with several months of worsening right upper and lower quadrant abdominal pain with radiation to the right anterior thigh accompanied by paresthesia and numbness. She also reported right-sided neck pain with numbness radiating into the right arm involving the ring and middle finger. Four months before this visit, she was treated with a cholecystectomy to address her abdominal pain: the gallbladder proved to be normal. Next, a computed tomography (CT) of the abdomen and pelvis demonstrated multiple lesions within the psoas muscle and mesentery of the lower abdomen [Figures




DISCUSSION
Genetics of NF-1
NF-1 is an autosomal dominant genetic disorder caused by a deletion mutation of the neurofibromin gene on chromosome 17.[
MRN
Over two decades, MRN has slowly become an important resource for the imaging and diagnosis of many peripheral nerve disorders. Additionally, three-dimensional reconstructions of neurography images had markedly improved over this period, and is now being used more frequently.[
MRN as a diagnostic modality
MRN-based radiographic signs have been named, such as the “bag-of-worms” in the case of plexiform neuromas.[
CONCLUSION
MRN is an imaging modality specifically designed for visualization of peripheral nerves. Here, MRN identified NF-1 in a patient presenting with multiple neurofibromas in both the right brachial plexus, and lumbar plexus. On the basis of multiplicity of disease, it was elected to pursue nonsurgical management in this patient.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Ahlawat S, Chhabra A, Blakely J. Magnetic resonance neurography of peripheral nerve tumors and tumorlike conditions. Neuroimaging Clin N Am. 2014. 24: 171-92
2. Bhargava R, Parham DM, Lasater OE, Chari RS, Chen G, Fletcher BD. MR imaging differentiation of benign and malignant peripheral nerve sheath tumors: Use of the target sign. Pediatr Radiol. 1997. 27: 124-9
3. Chhabra A, Andreisek G, Soldatos T, Wang KC, Flammang AJ, Belzberg AJ. MR neurography: Past, present, and future. AJR Am J Roentgenol. 2011. 197: 583-91
4. Easton DF, Ponder MA, Huson SM, Ponder BA. An analysis of variation in expression of neurofibromatosis (NF) type 1 (NF1): Evidence for modifying genes. Am J Hum Genet. 1993. 53: 305-13
5. Evans DG, Howard E, Giblin C, Clancy T, Spencer H, Huson SM. Birth incidence and prevalence of tumor-prone syndromes: Estimates from a UK family genetic register service. Am J Med Genet Part A. 2010. 152A: 327-32
6. Li CS, Huang GS, Wu HD, Chen WT, Shih LS, Lii JM. Differentiation of soft tissue benign and malignant peripheral nerve sheath tumors with magnetic resonance imaging. Clin Imaging. 2008. 32: 121-7
7. Maravilla KR, Bowen BC. Imaging of the peripheral nervous system: Evaluation of peripheral neuropathy and plexopathy. AJNR Am J Neuroradiol. 1998. 19: 1011-23
8. Mauermann ML, Amrami KK, Kuntz NL, Spinner RJ, Dyck PJ, Bosch EP. Longitudinal study of intraneural perineurioma—a benign, focal hypertrophic neuropathy of youth. Brain. 2009. 132: 2265-76
9. Peltonen S, Kallionpaa RA, Peltonen J. Neurofibromatosis type 1 (NF1) gene: Beyond cafe au lait spots and dermal neurofibromas. Exp Dermatol. 2017. 26: 645-8
10. Seddon HJ, Medawar PB, Smith H. Rate of regeneration of peripheral nerves in man. The J Physiol. 1943. 102: 191-215
11. Soldatos T, Andreisek G, Thawait GK, Guggenberger R, Williams EH, Carrino JA. High-resolution 3-T MR neurography of the lumbosacral plexus. Radiographics. 2013. 33: 967-87
12. Sunderland S. A classification of peripheral nerve injuries producing loss of function. Brain. 1951. 74: 491-516
13. Wallace MR, Marchuk DA, Andersen LB, Letcher R, Odeh HM, Saulino AM. Type 1 neurofibromatosis gene: Identification of a large transcript disrupted in three NF1 patients. Science. 1990. 249: 181-6
14. Wasa J, Nishida Y, Tsukushi S, Shido Y, Sugiura H, Nakashima H. MRI features in the differentiation of malignant peripheral nerve sheath tumors and neurofibromas. AJR Am J Roentgenol. 2010. 194: 1568-74
15. Yuh EL, Jain Palrecha S, Lagemann GM, Kliot M, Weinstein PR, Barbaro NM. Diffusivity measurements differentiate benign from malignant lesions in patients with peripheral neuropathy or plexopathy. AJNR Am J Neuroradiol. 2015. 36: 202-9

