

- Department of Neurosurgery, Max Super Speciality Hospital, Saket, New Delhi, India
- Department of Neurointervention, Max Super Speciality Hospital, Saket, New Delhi, India
- Department of Neurology, Max Super Speciality Hospital, Saket, New Delhi, India
Correspondence Address:
Saraj K. Singh
Department of Neurology, Max Super Speciality Hospital, Saket, New Delhi, India
DOI:10.4103/sni.sni_68_18
Copyright: © 2018 Surgical Neurology International This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.How to cite this article: Singh SK, Agarwal H, Singh P, Goel K. Intraventricular metastasis mimicking meningioma. Surg Neurol Int 26-Jul-2018;9:149
How to cite this URL: Singh SK, Agarwal H, Singh P, Goel K. Intraventricular metastasis mimicking meningioma. Surg Neurol Int 26-Jul-2018;9:149. Available from: http://surgicalneurologyint.com/surgicalint-articles/intraventricular-metastasis-mimicking-meningioma/
Date of Submission
02-Mar-2018
Date of Acceptance
12-Jun-2018
Date of Web Publication
26-Jul-2018
A 69-year-old male patient presented with multiple episodes of fall for 6 months. Magnetic resonance imaging of the brain showed T1 isointensity, T2 hyperintensity, and homogenous enhancement on contrast [Figure
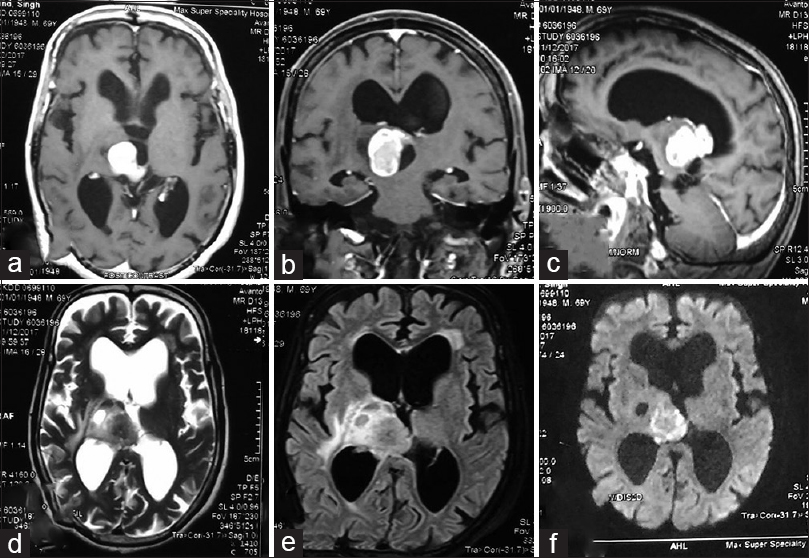
Figure 1
(a-c) Contrast-enhanced brain MRI (axial, coronal and sagittal sequences, respectively) showing homogenously enhancing lesion at the posterior third ventricular region. (d) Axial T2 brain MRI sequence showing hyperintense mass attached to tela choroidea. (e) FLAIR sequence of brain MRI showing hyperintense lesion. (f) DWI sequence of brain MRI showing diffusion restriction in the lesion
Intraventricular metastasis presents with various aspects of enhancement (uniform, punctate, ring) which can often lead to misdiagnosis of meningioma.[
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Tagle P, Villanueva P, Torrealba G, Huete I. Intracranial metastasis or meningioma?. An uncommon clinical diagnostic dilemma. Surg Neurol. 2002. 58: 241-5
2. Brant WE, Helms CA.editors. Fundamentals of diagnostic radiology. Philadelphia: Lippincott Williams & Wilkins; 2007. p. 143-

