

- Department of Neurosurgery, Instituto Paulista de Referência, São Paulo, Brazil
- Department of Neurosurgery, Neurosurgery Resident of Hospital Beneficência Portuguesa de São Paulo - Equipe CENNA (Centro Especializado de Neurologia e Neurocirurgia Associados LTDA), São Paulo, Brazil
- Department of Neurosurgery, Neurosurgery Resident of Hospital Celso Pierro, PUC Campinas, Campinas, São Paulo, Brazil
Correspondence Address:
Juliano Nery Navarro
Department of Neurosurgery, Neurosurgery Resident of Hospital Celso Pierro, PUC Campinas, Campinas, São Paulo, Brazil
DOI:10.25259/SNI-32-2019
Copyright: © 2019 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Juliano Nery Navarro, Francisco de Assis Ulisses Sampaio, Mario Sergio Duarte Andrioli, Francisco Ricardo Ribeiro, Mariano Ebram Fiore, Bartolomeu Souto Queiroz Quidute, Maick Wilen Fernandes Neves. Spinal subdural hematoma after lumbar discectomy without dural injury – Is it possible? A case report and literature review. 24-Apr-2019;10:66
How to cite this URL: Juliano Nery Navarro, Francisco de Assis Ulisses Sampaio, Mario Sergio Duarte Andrioli, Francisco Ricardo Ribeiro, Mariano Ebram Fiore, Bartolomeu Souto Queiroz Quidute, Maick Wilen Fernandes Neves. Spinal subdural hematoma after lumbar discectomy without dural injury – Is it possible? A case report and literature review. 24-Apr-2019;10:66. Available from: http://surgicalneurologyint.com/surgicalint-articles/9288/
Date of Submission
12-Dec-2018
Date of Acceptance
15-Jan-2019
Date of Web Publication
24-Apr-2019
Abstract
Background:Spinal subdural hematoma (SSDH) is a rare complication of lumbar discectomy. Here, the authors reviewed 10 articles concerning the etiology, clinical, diagnostic, and surgical management of SSDH.
Case Description:A postoperative SSDH occurred following a lumbar microdiscectomy in an 80-year-old patient in the absence of a dural injury.
Conclusion:SSDH is a rare complication of lumbar discectomy and may even occur without a dural fistula. Notably, magnetic resonance is the diagnostic study of choice to identify this pathology that may then be appropriately managed.
Keywords: Hematoma, lumbosacral region, postoperative period, subdural
INTRODUCTION
Spinal subdural hematomas (SSDHs) are rare following lumbar diskectomy; they account for just 4.1% of all spinal hematomas, and in 5% of cases, there is no evidence of any clear-cut cause.[
SSDH may occur due to multiple factors; vascular malformation, tumors, bleeding disorders, anticoagulant therapy, trauma, and infection but has only rarely been described after diagnostic lumbar punctures and/or spinal anesthesia.[
Here, we report a case of SSDH following a lumbar microdiscectomy without accompanying dural injury.
CASE DESCRIPTION
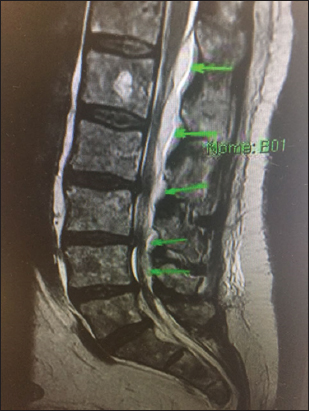
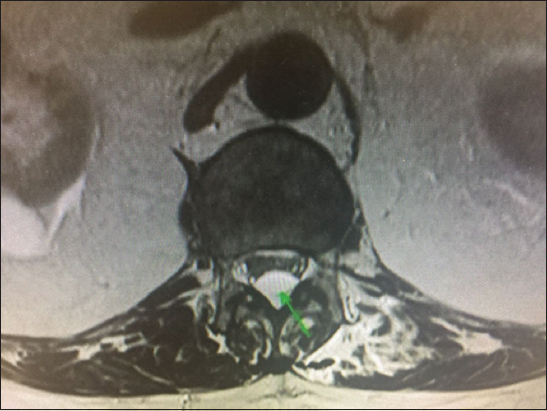
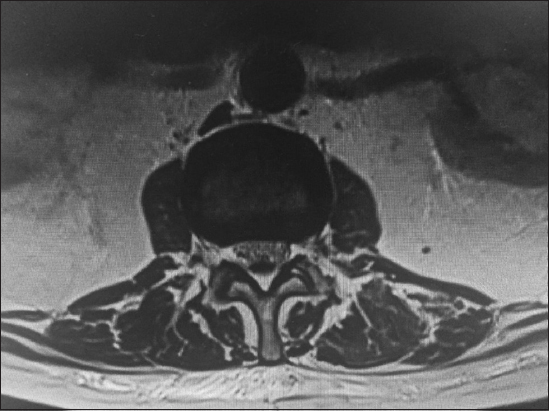
An 80-year-old male complaining of the left lumbar pain underwent a magnetic resonance (MR) scan that documented a herniated lumbar disc on the left at the L4–L5 level. He underwent an L4–L5 hemilaminectomy/microdiscectomy, without a dural fistula. Notably, he had stopped acetylsalicylic acid (ASA) utilized for an aortic valve prosthesis, 4 days before surgery.
Immediately postoperatively, he complained of bilateral lower extremity numbness. The lumbar MR scan revealed an acute SSDH extending from L1 to S1 [Figures

DISCUSSION
Gehri et al. first described SSDH as a complication of spinal surgery in 2000. They highlighted these lesions typically resulted from a dural tear during microdiscectomy.[
Chang et al. reported a 59-year-old female who following an L3–L5 laminectomy with instrumentation and fusion developed an acute MR documented SSDH at the L2 level proximal to the laminectomy.[
Lykissas et al. published two cases of acute SSDH after lumbar decompressive surgery, one of whom had an incidental durotomy.[
A prospective study at the Twin Cities Spine Center, Minneapolis, MN, USA, (2008) showed that lumbar decompression surgery results in a 58% incidence of asymptomatic compressive postoperative epidural hematoma (POEH). Adjacent level compression by POEH occurs in 28% of patients. Advanced age (>60), multilevel procedures, and preoperative international normalized ratio were independently associated with POEH.[
A recent study involved a retrospective analysis of the MR images of 410 patients who underwent lumbar decompression surgery with or without instrumented fusion to assess the prevalence and risk factors for spinal subdural lesions (SSDLs). They identified SSDLs in 30% of the 410 cases of lumbar spine surgery.[
Mattei et al. reported a case of acute SSDH after vertebroplasty.[
de Beer et al. showed that spontaneous SSDHs were predominantly located in the thoracic spine and correlated with acute paraparesis/paraplegia; over 40% was caused by a coagulation defect, most frequently due to Coumadin.[
On study (2015) documented a mortality rate of approximately 1.3% and a morbidity rate (permanent neurological deficits) of 28% for patients with SSDH.[
Two risk factors may also contribute to SSDH in the case reported here: age >60 years and the prior use of ASA.
Surgical recommendation
Emergency evacuation through durotomy is the treatment of choice to treat SSDH with neurologic impairment. Conservative management may be indicated in selected cases with clinical improvement and without significant motor/sensory deficits.
CONCLUSION
SSDH is a rare complication of lumbar discectomy. For patients acutely presenting with pain and/or other new postoperative deficits may have SSDH best documented with MR studies. Conservative care may be warranted for minimally symptomatic patients, while decompressive surgery may be required for those with significant neurological findings.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Chang KC, Samartzis D, Luk KD, Cheung KM, Wong YW. Acute spinal subdural hematoma complicating lumbar decompressive surgery. Evid Based Spine Care J. 2012. 3: 57-62
2. de Beer MH, Eysink Smeets MM, Koppen H. Spontaneous spinal subdural hematoma. Neurologist. 2017. 22: 34-9
3. Gakhar H, Bommireddy R, Klezl Z, Calthorpe D. Spinal subdural hematoma as a complication of spinal surgery:Can it happen without dural tear?. Eur Spine J. 2013. 22: S346-9
4. Gehri R, Zanetti M, Boos N. Subacute subdural haematoma complicating lumbar microdiscectomy. J Bone Joint Surg Br. 2000. 82: 1042-5
5. Lykissas MG, Aichmair A, Herzog RJ, Schroeder JE, Huang RC, Farmer J. Spinal subdural hematoma following lumbar decompressive surgery:A report of two cases. Wien Klin Wochenschr. 2015. 127: 71-4
6. Mattei TA, Rehman AA, Dinh DH. Acute spinal subdural hematoma after vertebroplasty:A Case report emphasizing the possible etiologic role of venous congestion. Global Spine J. 2015. 5: e52-8
7. Nagamoto Y, Takenaka S, Aono H. Postoperative spinal subdural lesions following lumbar spine surgery:Prevalence and risk factors. Asian Spine J. 2017. 11: 793-803
8. Pereira BJ, de Almeida AN, Muio VM, de Oliveira JG, de Holanda CV, Fonseca NC. Predictors of outcome in nontraumatic spontaneous acute spinal subdural hematoma:Case report and literature review. World Neurosurg. 2016. 89: 574-70000000
9. Sakai T, Sairyo K, Bhatia NN, Miyagi R, Tamura T, Katoh S. MRI changes of the spinal subdural space after lumbar spine surgeries:Report of two cases. Asian Spine J. 2011. 5: 262-6
10. Sokolowski MJ, Garvey TA, Perl J, Sokolowski MS, Cho W, Mehbod AA. Prospective study of postoperative lumbar epidural hematoma:Incidence and risk factors. Spine (Phila Pa 1976). 2008. 33: 108-13


JAIME TRUEBA
Posted May 6, 2019, 2:58 pm
I haven’t had any cases of subdural hematoma after lumbar discoidectomia. But if epidural, secondary to severe bleeding of peridural plexus, deficit coagulation by use of NSAIDs for long time, prior to surgery. Even with normal clotting studies.