

- Department of Orthopaedics, Changi General Hospital, Singapore
- Department of Pathology, Changi General Hospital, Singapore
Correspondence Address:
Sourabh Chachan
Department of Orthopaedics, Changi General Hospital, Singapore
DOI:10.4103/sni.sni_120_17
Copyright: © 2017 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Sourabh Chachan, H. R. Bin Abd Razak, W. Lim Loo, C. Sheng Tan, S. K. Dinesh. Extradural hemangioma mimicking a dumbbell nerve sheath tumor in the thoracolumbar spine: Case report. 10-Oct-2017;8:244
How to cite this URL: Sourabh Chachan, H. R. Bin Abd Razak, W. Lim Loo, C. Sheng Tan, S. K. Dinesh. Extradural hemangioma mimicking a dumbbell nerve sheath tumor in the thoracolumbar spine: Case report. 10-Oct-2017;8:244. Available from: http://surgicalneurologyint.com/surgicalint-articles/extradural-hemangioma-mimicking-a-dumbbell-nerve-sheath-tumor-in-the-thoracolumbar-spine-case-report/
Date of Submission
05-Apr-2017
Date of Acceptance
17-May-2017
Date of Web Publication
10-Oct-2017
Abstract
Background:Extradural hemangiomas are rare, have varied and challenging clinical presentations, and require special considerations from the management point of view.
Case Description:A 70-year-old female presented with back pain that was ultimately attributed to a thoracolumbar extra-dural “dumbbell” hemangioma. Following surgical resection, the patient did well.
Conclusion:Extradural hemangiomas may present as spinal extradural soft tissue masses that must be differentiated from dumbbell neurofibroma.
Keywords: Extradural hemangioma, nerve sheath tumor, thoracolumbar spine
INTRODUCTION
Hemangiomas are congenital vascular malformations of unknown etiology.[
CASE REPORT
Clinical presentation and magnetic resonance/computed tomography findings
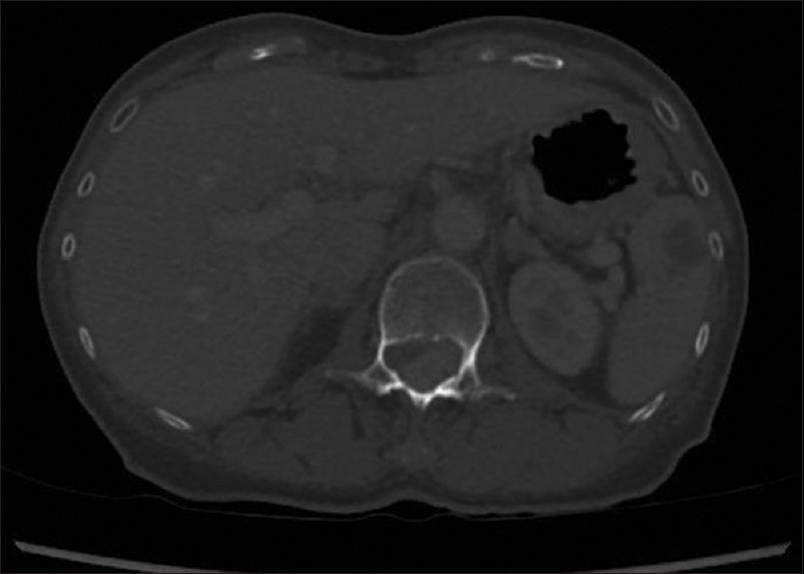
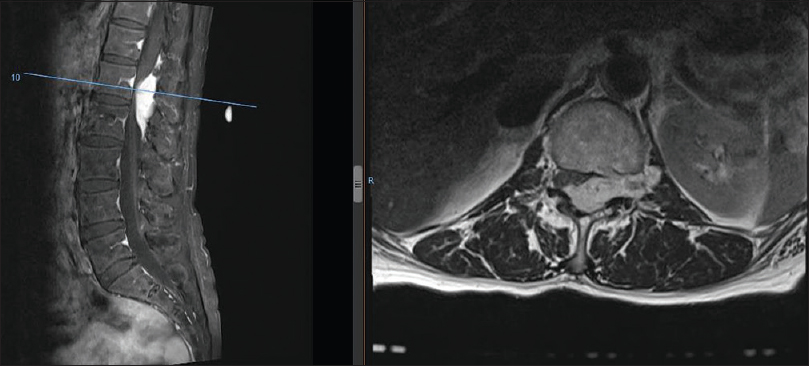
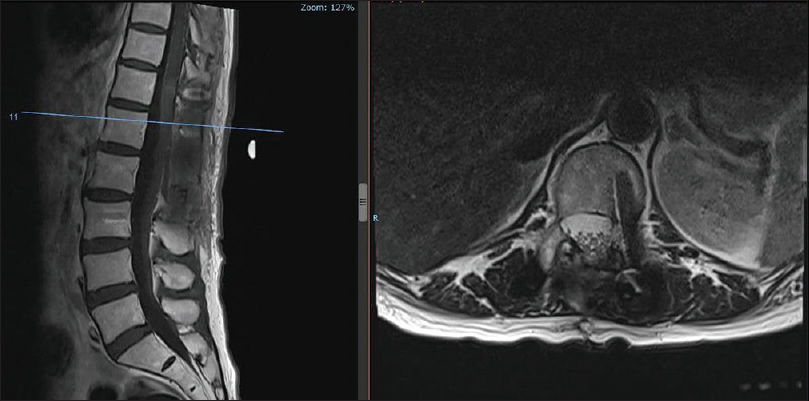
A 70-year-old Chinese female presented with deep-seated epigastric pain radiating to the back/flanks without a focal neurological deficit. The esophagogastroduodenoscopy was negative. The patient underwent computed tomography (CT) scan of the abdomen/pelvis, which documented an enhancing extradural spinal lesion measuring approximately 2.3 × 1.5 cm at the level of the L1 and L2 vertebrae, resulting in severe central canal stenosis [
Surgery
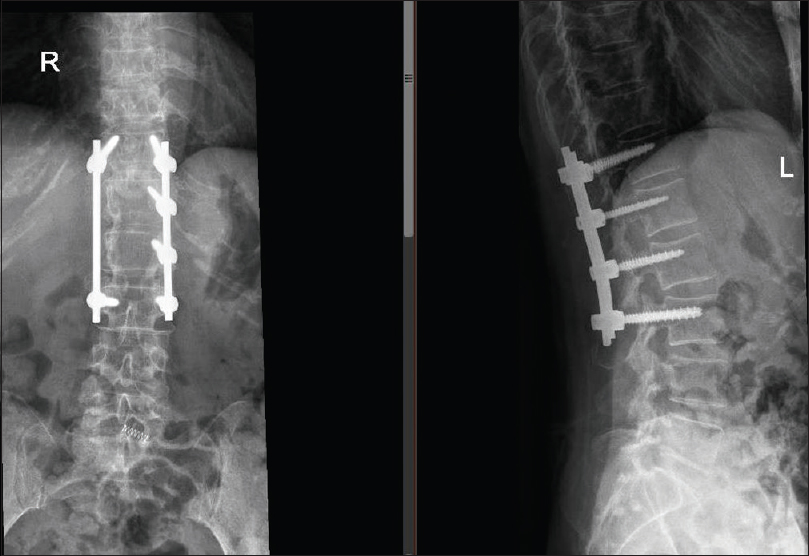
The patient underwent T12–L3 laminectomy with L1–L2 left facetectomy for excision of the tumor accompanied by T12–L3 instrumented fusion [
Histology
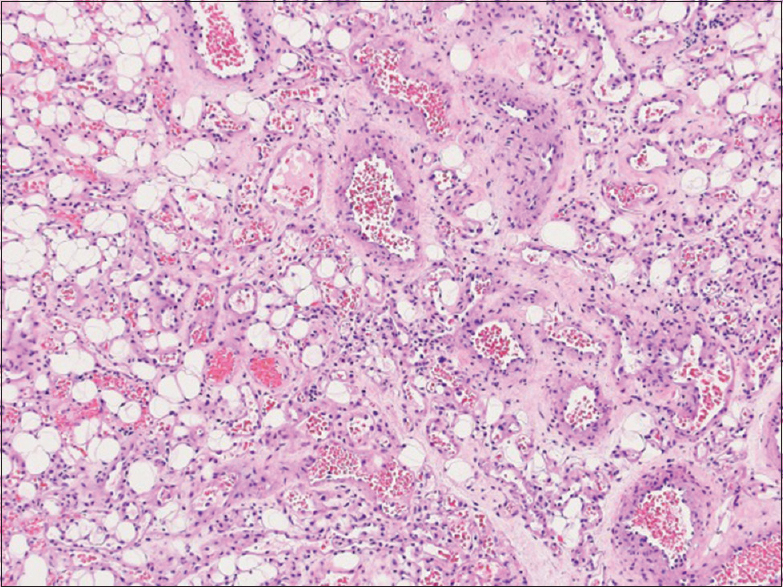
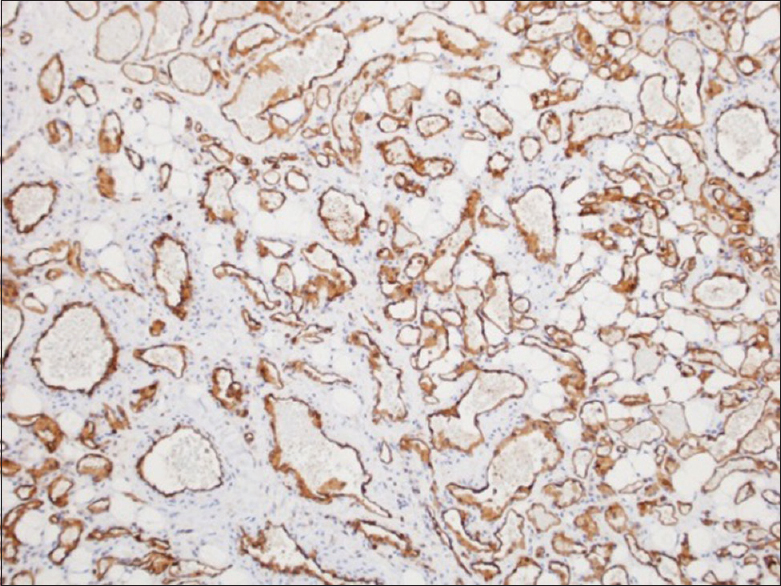
Histological examination showed fibroadipose tissue with diffuse proliferation of densely packed vascular channels closely associated with some arterioles and venules without any thrombosis [
Postoperative course
Four months after the surgery, the patient remained neurologically intact. MRI repeated 3 months postoperatively showed complete resection of tumor and no cord compression [
DISCUSSION
Extradural hemangiomas are rare, and are characteristically slowly progressive lesions that rarely present with acute neurological deterioration.[
The most common differential diagnoses include schwannoma, lymphoma, meningioma, angiolipoma, disk herniation, synovial cysts, granulomatous infection, pure epidural hematoma, and extramedullary haematopoiesis.[
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Aggouri , M , Berete I, Himmich M, Chakour K, Chaoui MF. Extradural Hemangioma of Thoracic Spine. Open J Mod Neurosurg. 2014. 4: 190-2
2. Badinand B, Morel C, Kopp N, Tran Min VA, Cotton F. Dumbbell-shaped epidural capillary hemangioma. AJNR Am J Neuroradiol. 2003. 24: 190-2
3. Lee JW, Choo EY, Hong SH, Chung HW, Kim JH, Chang KH. Spinal Epidural Hemangiomas: Various Types of MR Imaging Features with Histopathologic Correlation. AJNR Am J Neuroradiol. 2007. 28: 1242-8
4. Minh NH. Cervicothoracic spinal epidural cavernous hemangioma: Case report and review of the literature. Surg Neurol. 2005. 64: 83-5
5. Weiss SW, Goldblum JR.editors. Benign tumors and tumor-like lesions of blood vessels. Weiss's Soft Tissue Tumors. St Louis: Mosby; 2001. p. 837-90

